Janet Rossant is the president and scientific director of the Gairdner Foundation, which bestows the Canada Gairdner Awards. She is also a professor in Temerty Faculty of Medicine’s Department of Molecular Genetics, and the chief of research emeritus and senior scientist emeritus at The Hospital for Sick Children.
Over the course of more than 50 years as a scientist, I’ve held many roles.
One thing has never been clearer.
Now, more than ever, we must stand up for science.
As president of the Gairdner Foundation, I have consulted with colleagues around the globe, and we all agree — the scientific world must stand up and be heard right now.
Everywhere — and, in some places, more so than others — there’s an attack on the concept that research is important and that evidence matters. Science gave us penicillin, messenger RNA vaccines and Ozempic. All these advances came from fundamental research and novel methodology.
If we want to have healthier communities and to solve the big problems facing the world, the only way forward is with discovery and innovation.
Scientists and trainees at the University of Toronto, and the Toronto Academic Health Science Network, must be steeped in the understanding that science matters to society.
We also need to invest more in science.
For most of the last two decades, Canada’s national spending on research and development has not surpassed two per cent of its GDP — well below the average for members of the Organisation for Economic Co-operation and Development.
And yet, U of T placed fourth in the world for health sciences in the 2025 Nature Index, which measures research output by quality and volume.
We succeed despite ourselves, but imagine what we could do with more — more funding and collaboration, but also more diverse voices at the table.
When people with different backgrounds and experiences come together — which we do every day as Canadians — our work is more meaningful and achieves greater impact.
This requires us to reach out and encourage people in underserved communities to consider scientific or medical careers, to bring new energy and thought.
Ultimately, people around the world are looking to Canada and U of T to show that our country stands up for science. Let’s show them we believe in science, and that we see a clear way forward to a better future for all.
Then &
1970s
This photo of the late Ursula Franklin, one of Canada’s most famous scientists, is believed to have been taken in the 1970s. Franklin was a pioneering University of Toronto expert in archaeometry, the field of archaeological science, and the first female professor at what is now known as the Department of Materials Science and Engineering. In this photo, Franklin is working with an X-ray diffractometer, a machine for taking X-ray diffraction images of crystals. Photo: University of Toronto Archives
Now
2025
Atina Coté (PhD ’09), a senior research associate at the Donnelly Centre for Cellular and Biomolecular Research, works with a phase contrast microscope in Lea Harrington’s lab. Harrington (MSc ’90) is a professor and chair of the Temerty Faculty of Medicine’s Department of Biochemistry. Photo: Erin Howe
Photo of Daniel Drucker, taken by Polina Leif.
Safeguarding Science in Uncertain Times
By Betty Zou
Daniel Drucker (MD ’80, PGME ’84) is at the pinnacle of his career. Glucagon-like peptide-1 (GLP-1) medicines, such as Ozempic and Wegovy, are everywhere and are having a massive cultural moment thanks in part to Drucker, a professor at the University of Toronto’s Temerty Faculty of Medicine. Starting in the 1980s, he did the yeoman’s work that underpinned the development of these drugs.
Drucker, who started his scientific career more than 40 years ago, thinks we are currently living in a golden age of science. He also believes science is in crisis.
On both counts, he’s not wrong.
Thanks to decades of research advances, cellphones that double as powerful hand-held computers are now ubiquitous, and once-fatal diseases have transformed into manageable chronic illnesses. And, for better or worse, artificial intelligence (AI) is changing the way we work and live our lives.
And yet, science — and the people doing it — face growing threats from both outside and within the scientific community. Ideas that have been widely accepted as scientific consensus — that climate change is caused by human activity, that vaccines do not cause autism, that HIV causes AIDS — are being challenged because as a society, we can no longer agree on what constitutes a truth.
Scientists, health care professionals, learners and the institutions that support them are called upon to defend their work while also acknowledging and addressing the shortcomings of the current system.
What’s at stake in this fight? Credibility. Progress. Everything.
The righteousness of reproducibility
“My whole life, I have never wanted to be wrong,” says Drucker, a professor in Temerty Medicine’s Department of Medicine and a senior scientist at Sinai Health’s Lunenfeld-Tanenbaum Research Institute. “I know that sounds like the dumbest thing because no one wants to be wrong. But in science, you must bend over backwards to get it right because it’s an obligation we have to the people who are funding the work.”
What makes Drucker unique is not his commitment to careful, curiosity-driven science, but the lengths to which he is willing to go to ensure the reproducibility of findings from both his lab and the larger field of diabetes research, where his work on GLP-1 has had the biggest impact.
When someone in his lab shares a particularly exciting result with him, he often asks another lab member to try and independently replicate the experiment. He’s also known to call out colleagues and journal editors on X (formerly Twitter) when he spots something that’s not quite right — a privilege that comes with his seniority and reputation in the field, and one that has cost him friends and made him enemies.
As a clinician scientist, Drucker is motivated by his patients to be laser-focused on translating discoveries made in the lab into new treatments that improve human health. His pioneering work on the gut hormone glucagon laid the foundation for two new classes of drugs for type 2 diabetes and obesity, and a new treatment for short bowel syndrome.
He sees irreproducibility — across biological traits such as sex and age, from animals to humans, or between labs — as a major challenge that’s slowing down progress not just in his field, but in biomedical research at large. There have not been a lot of comprehensive studies examining the degree of reproducibility across biomedical fields, but the data that do exist are disheartening.
In 2021, a massive eight-year collaborative effort to replicate experiments from high-impact cancer biology papers found that just 46 per cent of replications successfully reproduced the results of the original experiment, a finding in agreement with earlier results from a similar reproducibility project in psychology. When the results did replicate, the effect size was significantly smaller than what was originally reported — half the magnitude in psychology and 85 per cent smaller in cancer biology.
More encouraging results from a retrospective analysis of 400 studies related to immunity in the Drosophila fruit fly found that 61 per cent of claims were verifiable. The findings were shared in two preprints posted to bioRxiv in July 2025.
Reproducible Open AI starts with open code
As a relatively young field, there is scant data on reproducibility in AI research, particularly as it applies to health and medicine. But that has not deterred Benjamin Haibe-Kains from calling for more transparency and openness in sharing the codes and data sets that are key to developing AI tools.
“One of the core principles of science is that it can be repeated, independently scrutinized and more importantly, reused and improved upon,” says Haibe-Kains, a senior scientist at University Health Network (UHN) and professor of medical biophysics at Temerty Medicine. “If you’re the only one who can generate a result, it has little to no value to humankind,” says Haibe-Kains, who is also the executive AI scientific director and co-director of the AI Hub at UHN.
His research aims to develop computational tools and predictive models that can leverage large data sets to improve our understanding of cancer biology and precision medicine approaches for people with cancer.
In 2020, Haibe-Kains and his colleagues wrote a commentary about a study led by a team of researchers at Google Health and DeepMind describing an AI system they created to interpret mammograms for breast cancer screening. The findings, which were published in Nature, claimed that the AI system was faster and more precise than the work of radiologists, outperforming human experts in certain settings.
While Haibe-Kains and his co-authors did not dispute the system’s potential, they wrote that “the absence of sufficiently documented methods and computer code underlying the study effectively undermines its scientific value.” In response, the study authors expanded the article’s supplementary methods with more, though still not complete, details.
Benjamin Haibe-Kains
Truth detectives
Many of the factors that contribute to an experimental finding being irreproducible are the result of what science integrity sleuth Dorothy Bishop calls “questionable research practices.” These include inappropriate statistical analysis (known as p-hacking), selective reporting, insufficient controls and small sample sizes.
“That’s not fraud,” says Bishop, who is an emeritus professor of developmental neuropsychology at the University of Oxford in England. “It’s people not doing things as they should because often, it’s become normative, and they haven’t been trained on how to do things properly.”
Like most of the sleuths she knows, Bishop fell into the hobby by accident in 2015 when she was tipped off about dubious activities at a journal. Initially, she investigated cases of questionable research practices, but over the past five years, she has seen a precipitous increase in what she describes as “industrial-scale fraud” in the scientific publishing industry.
These include paper mills that churn out low-quality, AI-generated papers where for a price, anyone can be listed as an author, and predatory journals that charge authors thousands of dollars to publish a paper with the promise of fast and less-than-rigorous peer review. More recently, the work of Bishop and her fellow sleuths has uncovered what she calls “review mills,” coordinated networks of reviewers who provide generic and often fake reviews to coerce authors to cite the reviewers’ own papers.
The not-so-glamorous side of science
While the line between sloppy science and deliberate misconduct can sometimes get blurred, these actions are all driven by the same unrelenting pressure to publish. Job appointments, promotions, awards, funding, university rankings — so much of it hinges on how often you publish, where you publish and how many other people cite your publications.
Making matters worse, federal spending on research in Canada has fallen short of both inflation and the demand for innovation. According to data from the World Bank, Canada is the only country in the G7 to have had its gross domestic spending on research and development decline between 2002 and 2022. During that same timeframe, funding success rates at the Canadian Institutes of Health Research were cut nearly in half from an average of 31 per cent in 2000–2003 to 17.5 per cent in the 2022–2025 competitions.
The pressures of this system are most strongly felt by early-career researchers — postdoctoral fellows trying to land their first academic job and junior faculty working to secure tenure, says Drucker.
It’s a struggle that Jinglin Lucy Xie (PhD ’17) knows all too well. Xie is a postdoctoral fellow at Stanford University in California who has been on the job market for the last several years, seeking a research faculty position. While she has gotten a few interviews, none have led to a job offer. When she looks at the profiles of the candidates who are making it through the hiring process, they often have a paper in one of the three so-called “glam journals” Nature, Cell or Science.
Xie believes that not having a first-author publication in one of these journals puts her at a significant disadvantage. When we speak, she is rushing to put the finishing touches on a resubmission to Nature just days before the due date of her second child.
“I care more about telling a coherent and compelling story of our discoveries than about whether it’s published in Nature, Cell or Science,” she says. Xie’s resolve to stay true to herself and to the science has meant at times pushing back on including data that would have made the story more exciting, but had not been replicated enough times for her to be confident in the results.
Even for Drucker, who received the 2025 Breakthrough Prize in Life Sciences for his work on GLP-1, publication in these top-tier journals was sometimes out of reach. He notes that the three discoveries from his lab that led to new classes of drugs were all published in PNAS, a respectable but less coveted journal.
“We couldn’t get into Nature, Science or Cell because we didn’t have spectacular and cool enough data for those journals,” he says.
Making enemies and progress
In a system that rewards quantity over quality and favours eye-catching, flashy headlines over meticulous, incremental advances, it’s perhaps not surprising that irreproducibility and fraud have emerged as major threats to scientific integrity.
“You get what you incentivize, and right now, we are incentivizing the wrong things,” says Drucker.
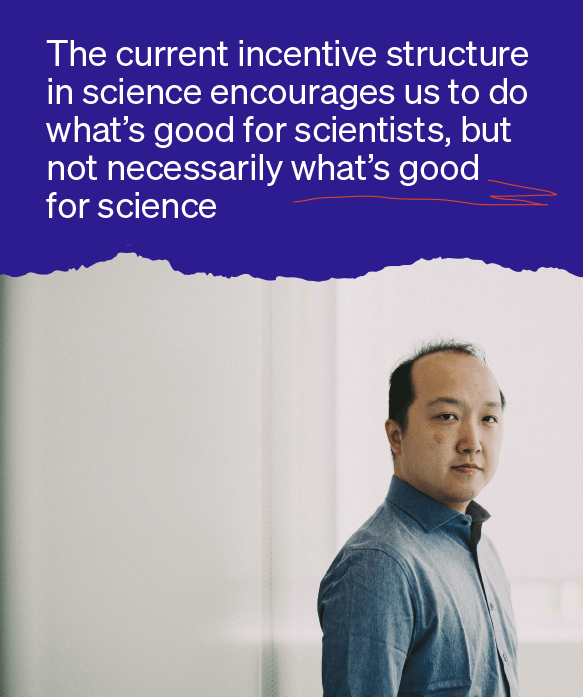
Felix Cheung agrees.
“The current incentive structure in science encourages us to do what’s good for scientists, but not necessarily what’s good for science,” he says.
Metascience — or as Cheung explains it, “the scientific study of how science works” — is trying to change that by bringing the two closer in alignment.
Now an assistant professor of psychology at U of T’s Faculty of Arts & Science, Cheung was drawn to the metascience movement as a young idealistic graduate student. He started graduate school in 2010, when concerns about a reproducibility crisis in psychology were at a peak. That motivated him to sign up to help replicate one of 100 studies tested in the Reproducibility Project: Psychology.
Cheung recalls the lengths to which he and his colleagues went to replicate the original experiment, including accounting for details, such as room layout and décor, that were not in the published manuscript. Despite their best efforts, they were unable to reproduce the results from the original experiment. Their results triggered heated exchanges that played out on X and in science and mainstream media.
Cheung remembers a comment from a professor at Harvard University who said that only second-rate researchers do replication studies because first-rate researchers conduct novel research.
“There were senior researchers at the time who tried to convince me not to pursue metascience research to ensure my own survival in the discipline,” he says. “When I started to make enemies, that’s when I realized that I’m standing up for something important.”
Today, he has found allies who share his commitment to improving science and is encouraged by the progress he’s seen in his field and others. For example, when he joined U of T’s faculty in 2020, he was heartened to see that the reproducibility project was already being taught as part of the undergraduate curriculum in psychology.
More journals and funders are requiring researchers to pre-register their studies, a practice that Cheung and his trainees already follow to reduce bias in reporting and analysis. Some journals are incentivizing reproducibility by publishing replication studies.
Felix Cheung
Shifting the culture of science
Every scientist you talk to will have a different idea of what is needed to make science more rigorous and trustworthy.
Drucker advocates for reproducibility to be included as a metric in promotion and funding applications, as well as for the publication of negative results. Haibe-Kains has created tools to help researchers share large biomedical data sets and to help institutions track their open science contributions. But they all agree that fundamentally, the culture within science must change.
“To change that culture, it has to come from putting the right incentives in place,” says Haibe-Kains.
Some of that change has already started. Bishop, who played a key role in establishing the UK Reproducibility Network, says that in the United Kingdom and Europe, funders typically ask for an applicant’s best or most impactful publications, making it easier for researchers to focus on the quality of their work rather than the quantity.
Xie notes that in the United States, all graduate students and postdoctoral fellows at institutions that receive funding from the National Institutes of Health are required to take courses on the responsible conduct of research.
In Canada, the Canadian Institutes of Health Research has mandated a course on research ethics for anyone whose research involves human participants, but there are no other requirements for trainees. Some institutions have stepped in to fill that gap, but the efforts have been piecemeal. Temerty Medicine’s Office of the Vice Dean, Research and Health Education, for example, offers a graduate research integrity workshop.
“Sometimes people step on ethical boundaries because they are naive about certain aspects of research ethics,” says Xie. “These courses increase awareness so that even if their supervisor doesn’t mention it, trainees still think about it.”
Concerns about reproducibility and misconduct in science are not new. What makes this moment different is the politicization of these issues and how they have been weaponized as an excuse to defund universities and strip away support for research across a range of disciplines.
“I feel conflicted, but we have to keep doing it,” says Bishop about her efforts calling out cases of misconduct. She worries that if fraudulent activities continue unchecked, science will become more insular as trust in science deteriorates among both the general public and within the scientific community itself.
Bishop says she is already hearing from researchers who are less willing to trust studies from Russia, China, Iran and other countries where paper mills have reportedly been found. And if the crisis continues, there’s the risk of walking back the progress that’s been made to make science more inclusive and losing a whole generation of talented young researchers, she says.
As for Xie, she is taking a temporary break from the job search to care for her son, who was born at the end of August.
“I’m still hopeful,” she says. “I believe in my science and the story I have to tell. It’s a matter of me convincing other people, and I’m not willing to give up yet.” •
Photo: Kristin Musselman
With concerns about cost, delays and lack of transparency, some experts are questioning whether the peer review system needs change
By Scott Fotheringham
At its best, the peer review process has safeguarded the accuracy and legitimacy of scientists’ findings.
“Peer review is at the heart of the processes of not just medical journals but all of science. It is the method by which grants are allocated, papers published, academics promoted, and Nobel prizes won,” wrote Richard Smith, in the Journal of the Royal Society of Medicine.
Smith published these words nearly 20 years ago, but they still ring true today. Peer-reviewed articles remain the dominant way for verifying and sharing scientific results.
However, with growing concerns about cost, delays, bias and the lack of transparency — and the rise of open publishing models — some experts are questioning whether this foundational system needs an overhaul. Take transparency. How reviews of academic articles are conducted, and by whom, is often opaque. This raises questions about bias and the credibility of the review process.
Kristin Musselman, an associate professor in the Temerty Faculty of Medicine’s Department of Physical Therapy, argues that accountability would be enhanced if reviewers, who are usually anonymous, had their names published alongside their peer-review comments.
“Naming reviewers will benefit research and publishing,” says Musselman, a senior scientist at the KITE Research Institute. “It should hold reviewers accountable to do thorough, unbiased reviews. It will also give reviewers recognition for this valuable work.”
Then there’s the laggardly pace. Musselman has experienced challenges in the slow nature of the review process from three angles: as an author and reviewer, and as the associate editor for three journals.
“As an author, a big challenge is the length of time it takes to receive reviews,” Musselman says. “It typically takes six months or more, slowing our output and meaning our findings are not shared with the research community as quickly.”
Reviewer fatigue and a lack of meaningful incentives
“There’s also been an increase in the number of journals, both reputable and predatory,” says Michele Anderson, a professor in Temerty Medicine’s Department of Immunology and a senior scientist at the Sunnybrook Research Institute. “[Predatory journals] have a low bar for scientific integrity, existing primarily to make money from researchers who need citations. People publish in them because research for legitimate journals requires more funding and takes longer.”
As a reviewer, Musselman gets a handful of review requests every day. She chooses to review only appropriate papers from reputable journals, whereas many requests come from journals with dubious review and publishing practices — the so-called “predatory journals” — or aren’t even in her area of expertise.
“In my experience as an associate editor, it’s onerous to recruit reviewers,” Musselman says. “It can take a dozen requests to find one person, which honestly makes me not want to be a journal editor.”
Reviewing can be time and labour-intensive. One journal article estimated the amount of time spent by US-based reviewers providing feedback was worth US$1.5 billion in 2020, leading the researchers to refer to the reviews as a “billion-dollar donation.”
“Lack of incentives limits the number of reviewers,” Anderson says. “It’s unpaid labour that can be frustrating, especially as our own work suffers while we do this free service. The discount tokens that some journals offer are downright insulting.”
The pressure on researchers to publish frequently as the primary measure of success needs to end, she says.
“There should be sufficient expertise in an institution to judge scientific progress without having to get through the jungle that publishing has become,” she says.
Training for emerging researchers
One solution to remove weight from reviewers is to increase the supply of people who can help. Undertaking peer review can be a learning experience for new investigators while reducing a primary investigator’s workload, say those involved in the process.
Anderson advocates for a multi-journal college of reviewers to train early-career scientists similar to the pool of reviewers used for Canadian Institutes of Health Research (CIHR) grant applications. Members would undertake training, have supervised probationary reviews and commit to a minimum number of reviews annually.
“I train my graduate students and postdocs how to review a paper,” Anderson says. “When I get an appropriate request for peer review, I give a primer on how to review and examples of my reviews. Then, we go over their review line by line with my suggestions.”
The editorial team at Nature also encourages established researchers to co-review, on an equal footing, with a junior scientist in their lab or department.
“The early-career researcher is entered into our database as an equal reviewing partner, and they receive feedback from the editors about the utility of their reviews,” says Magdalena Skipper, the editor-in-chief of Nature and chief editorial advisor for the Nature portfolio. Since research rarely starts and ends with one paper, experiencing peer review helps researchers position steps in the process of discovery while appreciating the limitations of findings.
“Understanding how peer review works is instrumental to constructing stories, sharing research and emphasizing future directions from the research summarized in any one paper,” she says.
Science depends on openness
In addition to building review capacity, some journals are moving toward transparency, including Nature — which now publishes reviewer reports and author responses with all research papers.
“The conversation between reviewers and authors, mediated by an editor, leads to substantially better manuscripts and needs to be seen,” says Skipper. “Transparency showcases the important contribution reviewers make to scholarship.”
In addition to immediate benefits, Skipper points out that reviewers’ comments can provide information to address a post-publication issue, such as a question about research integrity. At Nature, transparent peer review does not involve disclosing reviewers’ identity, Skipper notes. As well, greater transparency is not always a perfect solution. Anderson says issues with transparency can include the fear of retaliation.
“Early-career researchers often feel at the mercy of established scientists and may hesitate to offer honest critiques for fear of giving offence. Retaliation can be especially damaging when it manifests as harsh reviews of grants or manuscripts, which can be career-threatening,” she says. “Given human nature, this perceived risk is entirely reasonable and should be treated as a central concern in efforts to make peer review more transparent.”
eLife, a not-for-profit, open-access online publisher for life sciences and biomedical research, has introduced an innovative peer review model. Every reviewed article is published and accompanied by a public review and any author responses. Articles can be modified, and public reviews updated, in a process eLife calls “publish-review-curate.”
“These are great first steps towards expecting that reviews are published everywhere,” Musselman says. “It provides early-career researchers with the opportunity to peruse reviews and see the type of comments they might get on their submissions. This allows them to address potential criticisms as early as when they’re planning a study.”
For Musselman, contributing to peer review is part of a researcher’s responsibility to their field. Therein lies the hope for the future, she says.
“Science depends on openness, not secrecy. Repairing peer review can ensure it continues to protect scientific integrity,” she says. •
Illustrations by Vicky Lin
Doing scientific work can be mind-bending, confounding and rife with challenges.
It can also be a rewarding quest that fills researchers with hope and excitement.
Five members of the Temerty Faculty of Medicine community were asked: Why do you stay in science?
Here, they express what keeps them engaged in the discipline.
Science is a blank canvas, holding equal potential to do good or cause harm. As both a researcher and a clinician, I feel a profound responsibility to ensure it is harnessed to improve lives. In the hospital, science is always present — in the treatments and diagnostics available to patients, and in the data that guide complex decisions.
Science empowers patients, offering them a measure of control in the face of serious illness — an invaluable gift. In my global health work, the data we generate provides foundational insights into the challenges faced by vulnerable communities. These findings not only quantify but also amplify struggles that are too often hidden. Science, therefore, is not only the foundation of my awareness of health inequities, but also how I hope to change them. To me, science is a source of empowerment, a tool for justice and a bridge to health equity.
Betel (Betty) Yibrehu is a fifth-year general surgery resident in Temerty Medicine’s Department of Surgery.
When I was little, I told everyone I wanted to be a doctor. I told people my dream was to save the world. I still think, deep down, most of us in medicine feel that way. I was drawn to science because I’ve always wanted to understand how things work, particularly in humans. Now, I study genomes and try to translate science into something human.
I stay in science because I believe in truth — the kind you question, test and pursue, even when it’s hard. And, because in a world where science is often politicized, defunded or dismissed, I believe this work matters.
Anushka Deshmukh is a second-year Master of Health Science student in Temerty Medicine’s Department of Molecular Genetics.
I’ve worked for National Defence as a physical therapist since 2005. I’m proud to be a civilian member of the Canadian Armed Forces physiotherapy team.
One area of research that fascinates me is how training-related injuries are the leading cause of disability, lost time and attrition from military groups worldwide. Current research shows that the most effective way to lower training-related injuries is military leadership-supported modified physical training.
The research my team focuses on is building cooperation between civilian scientists, trainers and military leaders on how best to apply research on modified physical training.
As a clinician-scientist, it’s a privilege to contribute to programs that bridge the gap between research and practice, and ultimately, improve our military’s operational readiness. I stay in science in order to serve those who serve.
Eric Robitaille (MSc ’04 & PhD ’15) is an assistant professor in Temerty Medicine’s Department of Physical Therapy.
My research engages personal support workers, community health workers and others whose contributions are often overlooked in care. Science allows me to work with communities to co-create educational programs that foster excellence and resilience. Universities and research hospitals must ensure that the entire health care workforce is supported and included in innovation, learning and discovery.
Scientific inquiry lets us confront structural inequities and develop solutions based on lived experience. I won’t leave science as long as I am committed to justice, inclusion and system transformation. It is a space where I can amplify under-represented voices, challenge deeply held norms about who deserves support, and help build a more responsive and equitable system.
Nicole Woods is a professor in Temerty Medicine’s Department of Family and Community Medicine and a senior scientist at the Wilson Centre for Research in Education. Woods is also the director of The Institute for Education Research at University Health Network.
George Mallory, who died in a valiant attempt to be the first to summit Mount Everest, was once asked why he wanted to climb the world’s highest mountain.
His response: “Because it’s there.”
Why do I stay in science? Because it’s there.
Artem Babaian is an assistant professor in Temerty Medicine’s Department of Molecular Genetics and the Donnelly Centre for Cellular and Biomolecular Research.
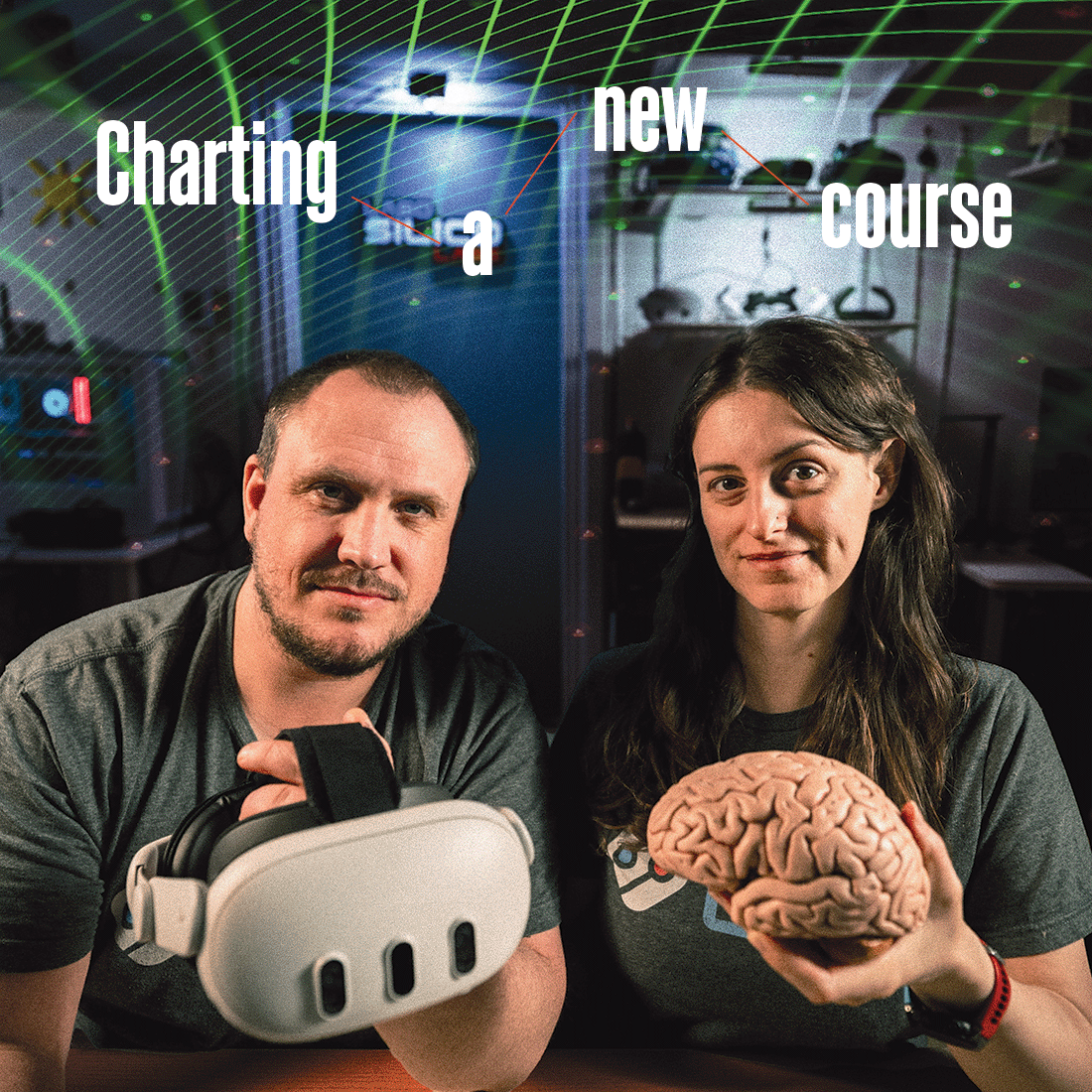
Photo: Kyla and Benjamin Alsbury-Nealy
By Erin Howe
What if the path you envisioned for yourself ended up taking you places you never expected?
That’s the case for Kyla Alsbury-Nealy (PhD ’24), who never imagined she’d co-found a software company and be its chief operating officer. A physiotherapist who had been in practice for four years, Alsbury-Nealy began working toward her doctorate in rehabilitation sciences at the University of Toronto Faculty of Medicine — now the Temerty Faculty of Medicine — in 2018.
Her goal was to advance patient care in her field through research and make an impact beyond what she could do for the patients she saw. But then, the road forked.
Although she loved her studies, midway through her degree, Alsbury-Nealy realized she wasn’t sure a career in academia was right for her. And she was disheartened by the idea that evidence from the studies she and her colleagues were doing might not make its way into practice for nearly 20 years.
“There’s so much important work underway, but it can take so long to help patients,” says Alsbury-Nealy. “One reason is that research can be quite abstract. We get people to fill out surveys or do interviews so we can understand their symptoms and experiences. That’s valuable, but there wasn’t a good way to simulate the real world to get rich behavioural information.”
Alsbury-Nealy and her husband, Benjamin Alsbury-Nealy, who was working toward his own PhD in cognitive neuroscience at U of T’s Faculty of Arts & Science at the time, found themselves thinking about ways to simulate real-world experiences to generate better data sets for their research.
With support from Temerty Medicine’s Health Innovation Hub, H2i; the Creative Destruction Lab at U of T’s Rotman School of Management; the U of T Early Stage Technology program, UTEST; and the U of T Entrepreneurship program, UTE, the pair established SilicoLabs in 2021. The company created a low-code/no-code platform that enables anyone to quickly and easily create experiences that researchers can use to capture rich data from hand and body movement, eye tracking, including pupil dilation and subtle shifts in facial expression.
Expectations about pathways after grad school are shifting, says Alsbury-Nealy. She’s just one graduate student who has forged an alternative path in a research-based career outside academia, thanks to better funding, new mentorship models, a culture that embraces entrepreneurship and flexibility — showing others the expanding possibilities of a career in research.
According to U of T’s School of Graduate Studies 2022 Career Outcomes Study, just 37.7 per cent of Temerty Medicine’s PhD graduates continue their careers in the post-secondary education sector.
Approximately 28 per cent obtained work in the private sector, and about 19 per cent more sought employment in the public sector, the study said.
While PhD graduates are employed in careers beyond academia, the traditional expectation for graduate students was to finish their education and become professors themselves.
Nana Lee (MSc ’95, PhD ’01) remembers how her own PhD supervisor reacted to the news that Lee would consider working in the private sector in biotechnology.: “What do you mean you’re going to the dark side!?” recalls Lee, now Temerty Medicine’s special advisor for graduate education and an associate professor in its Department of Biochemistry.
“At that time, around 25 years ago, the expectation was that graduate students would work toward careers in academia. There was no support for learners who wanted to explore other opportunities,” she says.
Despite leaving the world of higher education, Lee remained connected to her alma mater and returned in 2012 to speak to biochemistry students about her career trajectory. The department’s chair at the time, Professor Emeritus Reinhart Reithmeier, asked Lee if she wanted to work with him to create the faculty’s first graduate professional development credit course. About a dozen learners registered for the class, which empowered them to develop their communication skills, learn how to market themselves and reflect on their interests. Lee also invited a variety of guest speakers to share their experiences.
Since it was created, the course has been featured in the “Careers” section of Science, and Lee and Reithmeier published a University of Toronto Press book on the course. It has evolved and is now offered to both MSc and PhD students. Temerty Medicine’s Departments of Molecular Genetics, Pharmacology and Toxicology, Physiology and the Institute of Medical Science each have a curriculum-embedded iteration of the class tailored to their respective field.
“My peers and I didn’t have any of this stuff when we were ‘growing up.’ The culture has changed,” says Lee.
In addition to better preparing students for life beyond the lab, other developments have also helped ensure learners are better supported financially during their studies.
In fall of 2023, U of T and Temerty Medicine increased graduate student stipends. The move meant that students in the Master of Science programs would receive $37,000 annually, and PhD candidates would be offered $40,000 per year, the highest amounts in Canada. The following year, Canada’s federal government increased the value of scholarships for master’s and PhD students to $27,000 and $40,000 per year, respectively, as part of its budget.
During her student years, Kaitlin Kharas (PhD ’24) benefited from that financial boost and fought to extend the benefit to others. Kharas, who achieved her doctorate in Temerty Medicine’s Department of Laboratory Medicine and Pathobiology, says she recognized that government is the biggest funder of science, and that government relies on science and evidence to make good policies.
That push and pull led her to advocate for more money to support graduate students, noting the important role they play in contributing to scientific knowledge and the Canadian economy. Though she’s pleased with the progress she’s seen, Kharas says there’s more to be done.
“For a lot of graduate students across the country, funding is still an issue. Often, they’re still living at or below the poverty line. If someone is food or housing insecure, that has an impact not just on their quality of life, but also on their research,” says Kharas, who now works for an international consulting firm.
Taking on additional employment can cut into their time in the lab, Kharas points out.
Publication deadlines, grant applications and being present at key points in an experiment can be stressful, says Salma Sheikh-Mohamed (MSc ’20, PhD ’25), who completed her PhD in immunology in the spring.
“It’s the pressure of academia,” she says. “It’s like, ‘Everybody else is working, so I should be, too.’”
Sheikh-Mohamed began her PhD studies in the early months of the COVID-19 pandemic, adding to the fervour. Generally, she says, students spend the first 18 months or so learning techniques they’ll need for their research and determining which direction their studies will take.
But Sheikh-Mohamed got straight to work on trying to answer questions related to mucosal immune responses to vaccinations related to the serious, burgeoning virus. She remembers collecting vast amounts of data, attending conferences and publishing findings at an unexpected speed. At the time, there were just so many unknowns she and her colleagues were trying to answer. She credits her department chair, Professor Jennifer Gommerman (PhD ’98), for encouraging learners to take time for themselves and, if needed, take a brief step back from their research.
This fall, Sheikh-Mohamed started teaching undergraduate courses part-time. As a newly appointed assistant professor, she looks forward to being a mentor to her students and sharing some of the guidance she wishes she’d had at that stage.
“Being a grad student can feel like you’re on call 24-7. Sometimes you put in an incredible amount of work, and things don’t work out as planned. It’s just the nature of science,” she says. “It’s not a bad thing, but it helps to be prepared.”
And, when it comes to being prepared, Alsbury-Nealy notes that the intense nature of grad school prepared her for the demands of entrepreneurship. Today, she thinks of her work as being “academia adjacent.”
SilicoLabs supports research at top institutions in Canada, including U of T, and internationally, including KU Leuven in Belgium, the University of Cambridge in the United Kingdom and Stanford University in the United States.
“We’ve been able to have a broader impact than Benjamin or I had imagined,” she says. •
Illustration by Jud Haynes
Story by Alison Motluk
The message from Marla Shapiro’s patient was worrisome.
It began, “I’m pretty sure this is not you, but …”
The hesitation was because the patient had seen someone on Facebook who looked and sounded just like her. The person had the same name and was sitting in her home office. But the online double was peddling weight-loss gummies — something Shapiro would never do. The patient shared the link.
When Shapiro (MHSc ’83, PGME ’83), a professor in the Temerty Faculty of Medicine’s Department of Family and Community Medicine, watched the online video, she was stunned. There she was — her face, her voice, her expressions — saying things she would absolutely never say.
At the end of the short clip, which faithfully resembled a kind of television appearance she’d become famous for as CTV’s longtime medical expert, the video then took viewers to a website where they could purchase the product she was supposedly endorsing.
“I’ve had patients of mine who have gone ahead and just bought the gummies because they know me — they thought, ‘This is my doctor telling me about this amazing weight loss product,’” says Shapiro.
Her own husband thought the video looked like her. The problem? It wasn’t her.
Shapiro had been “deepfaked” — someone had used artificial intelligence (AI) to manipulate video to make her appear to be saying and doing things that were made up.
In recent years, politicians, celebrities, young women and even children have fallen victim to deepfakes of various kinds. Now, high-profile Canadian doctors are becoming targets too.
“It’s infuriating,” says Shapiro, “I work very hard to have this relationship with the public and to be a person who’s trustworthy. All that work is just trashed in moments in an AI posting.”
The problem didn’t go away. The video Shapiro watched that day almost two years ago was just one of many to come. Some appeared to be from her home office, some from CTV’s studio, and some included CTV’s chief anchor, Omar Sachedina. But as quickly as the fake videos were ordered to be taken down from one platform, they popped up on another.
Jim Mann, a professor in Medicine and Human Nutrition at the University of Otago in New Zealand, and a world-renowned diabetes expert, had a similar experience last year.
In a fake video, he appeared to be discussing a new “discovery” made by his team and “recommending” that diabetes patients abandon their current treatments in favour of a new product, which viewers could buy using the phone number provided. A neighbour saw the item and immediately knocked on his door to alert him.
Mann admits the deepfake sounded reasonably like him, though there were some giveaways: “I used the words ‘bloody idiot,’ which I have been known to use, but not on the national 6 o’clock news bulletin.”
Also, as with Shapiro, it was completely out of character for him to be touting a product this way. On balance, he says, he got more emails from people who recognized it as a fake, but it was nonetheless disturbing how many others were taken in, including people who knew him well. His university issued a press release about it and also notified the police, who said there was little they could do. A lot of time and effort was spent trying to stamp out the video and also to explain to patients and others what had happened.
But the same false video occasionally still resurfaces.
“The thing that disturbed me was that I’m a patron of the national diabetes organization, and I’ve worked in diabetes a long time, and subsequently discovered that this video was widely shown internationally,” he says.
So, what’s the greater public harm from deepfakes, beyond the distress and reputational hit to experts?
Fahad Razak (MD ’09, PGME ’13), an associate professor in Temerty Medicine’s Department of Medicine and the Canada Research Chair in Data-Informed Healthcare Improvement, says that the deepfaking of doctors and medical experts has suddenly become an important public health challenge. Only a few years ago, the advice on how to avoid fraudulent information was to trust government leaders, scientists and physicians.
“But, now that trust has fundamentally been undercut by deepfakes, because you don’t know if what you are seeing is actually that person,” he says. And that, he says, makes it harder to know where to go to get reliable science information. And it’s not like the issue is abating. There are hundreds of tools now widely available and being used, he says, to copy someone’s image and voice.
Earlier this year, Razak was in a meeting with Theresa Tam, then Canada’s chief public health officer, when a deepfake of her came to the group’s attention. The fake persona claimed she’d found rubberized clots during autopsies on people who’d been vaccinated against COVID-19, and then advocated for a product that would dissolve the clots in the still-living.
“It was a deepfake,” says Razak, “but it was a reasonably convincing one.”
Fake personas come not just in the form of videos. In 2024, someone created a fake X (formerly Twitter) account using Razak’s photo and affiliations and a name that was just one letter different from his own. The impersonators cleverly put a few fake but credible posts up top, he says, “and then quickly followed with personal outreach to people, trying to sell products.”
Fakes like these make it hard to know what the real experts are saying.
Then there’s the personal aspect.
Shapiro says she would like justice: “I’d like to have some recourse when someone puts something up that is not me, endorses something that I am not endorsing and dupes the public.” For now, however, the options are limited.
Technology evolves faster than the law, says Suzie Dunn, an assistant professor at the Schulich School of Law at Dalhousie University in Halifax and the director of its Law & Technology Institute. There has been some progress against deepfakes in some provinces, she says, where so-called “synthetic media” misuse is now treated the same way as real-image misuse. However, she notes that so far, new legislation only applies to cases in which the content is sexual in nature.
“There’s no example that I can point to that’s a perfect solution, and what Canada should be doing,” she says.
As far as she knows, there have been no deepfake lawsuits in Canada. But there are several ways deepfakes may be seen to contravene the law. For instance, deepfakes could be seen as fraud, she says. Alternatively, they could be seen as criminal impersonation.
Dunn also wonders if victims might be able to claim defamation: “This is false information that’s being put out publicly about a person,” she says, “that’s harming their reputation in the community.”
There are also privacy statutes that forbid someone from taking your image, name, voice and likeness and using it without your consent in a commercial context — often invoked by celebrities.
“I actually think this doctor form of deepfake impersonation fits really cleanly under that,” she says, “because it is a commercial enterprise.”
But you’d have to figure out who was behind it, bring a civil suit for appropriation of personality, and then ask for injunctions and damages. And often, the perpetrators are in faraway jurisdictions, she says. Plus, lawsuits are expensive and take time — months to years. More than anything, deepfake victims want the fake material taken down as quickly as possible.
Dunn points to another promising option: a civil resolution tribunal in which a person could bring evidence about a deepfake and have it quickly ordered to be taken down. British Columbia has established such a tribunal to help with intimate image deepfakes, says Dunn, and she wonders if the model could be broadened to include deepfakes of experts as well.
In the meantime, however, victims often resort to hiring “reputation managers” to scour the internet for fake videos or images and request that they be taken down, says Dunn. Many social media companies have rules around deepfakes and impersonations and, when confronted with evidence, will act.
“It’s such an important issue,” says Dunn. “I think we are seeing these things pop up a lot more. I can understand that fear those doctors have and that frustration with not really having a simple solution to something that’s a really big problem.”
Which means that for now, everyone will have to be especially vigilant.
“If the police and governments can’t do anything about it,” says Mann, “I think we need more awareness.” •
How to spot a deepfake?
Identifying what is real — and what is artificial — means evaluating online content with a critical eye.
Shion Guha, an assistant professor at the University of Toronto’s Faculty of Information and Department of Computer Science, shares some ways people may be able to recognize a deepfake video if they encounter one online.
It looks too perfect
Guha warns about what is known as “the uncanny valley.” The term refers to the idea that when computers, or robots or AI created images, they sometimes seem too realistic.
“When they seem too realistic, we understand it’s not reality,” he says.
To illustrate the term, Guha uses the example of a person in a deepfake whose skin has no blemishes, wrinkles or imperfections. Instead, it looks completely smooth.
“Anything that looks too perfect is probably a deepfake,” he says. “It’s something that is hard to quantify, but you know it when you see it.”
It has obvious flaws that sometimes flout reality
At the other end of the spectrum, Guha says a hint that something might be a deepfake is that it contains errors that simply aren’t possible (or are very, very rare) in real life.
As an example, Guha cites an image of a person not casting a shadow, or having a sixth toe or an orange eye.
“Sometimes, when AI generates an image, it is unable to generate it properly, so there are minute imperfections,” he says.
If there is sound, it sounds not quite right
A deepfake video with sound can also provide giveaways that it’s artificially generated. As an example, Guha recalls a video taken at night in which a fake sound of crickets echoes in the background at absolutely regular intervals.
Guha’s general principle is that people should be “extremely skeptical” when evaluating content online. He says it should especially be considered suspicious if it’s trying to convince the viewer to “do something they would not normally do” — such as buying something they wouldn’t normally buy or sharing private information.
“If you think something is fake, you should assume that it is fake,” he says.
Documenting research
Perspectives on curiosity-driven filmmaking
Through their upcoming CBC Gem documentary Doctor, doctor, U of T graduates Jonathan Qu and Kevin Li look behind the scenes at what goes into scientific discovery. Inspired by a desire to show what researchers experience as they work to establish new knowledge, Qu and Li shine a spotlight on Temerty Medicine Professors Andrew Sage and Kazuhiro Yasufuku and their efforts to improve lung cancer care.
Three researchers with the Temerty Faculty of Medicine address why equity in science and medicine is more important than ever, and why they make it a foundation of their work.
It lowers barriers for scientists
I’m a molecular bacteriologist who spends a lot of my time in a lab. But another big part of my life is the work I do to support queer and LGBTQ+ researchers.
As a young researcher, I didn’t know anyone like myself — a queer, gay man in science. When I did my PhD at another university, there was no one I knew who was out. In a very fundamental basic science department, I felt alone. That’s why I started building community and networks to meet other queer people in science, technology, engineering and math (STEM), and I’ve continued that work since I’ve moved to Toronto.
In 2023, I launched Pride in Microbiology with two other colleagues. Our network now has more than 200 members worldwide. As my colleagues and I explained in our launch article in Nature Microbiology, queer people in STEM face additional barriers compared with their peers.
Research shows queer people are more likely to switch out of a STEM-related undergraduate degree to a non-STEM field, and are also more likely to report feeling socially marginalized, professionally devalued, and having limited career opportunities, once on the job. This research tells us that we’re limiting and losing people who might be able to provide innovative ideas because of the culture of the space. And we’re failing talented minds because we’re not as supportive as we need to be.
If you come to work every day not feeling comfortable, and people do not treat you well, and you constantly face systemic barriers that prevent you from seeking mentorship or having the same opportunities as your peers, then you’ll be less engaged with the work you’re there to do.
When we think about strengthening innovation and discovery, it’s about ensuring people can come to a workplace where they feel respected, valid and comfortable, so their focus is on their studies and goals rather than overcoming additional barriers to their success.
I advocate for queer and LGBTQ+ people because it’s the right thing to do, and because it strengthens science.
Landon Getz is a postdoctoral fellow in Temerty Medicine’s Department of Biochemistry.
It serves the under-represented
Right now, science benefits some portions of society better than others.
Researchers are often trained to approach their work with an ethical focus on the protection of individuals. While that is absolutely necessary, it is not the focus of what I do. My research is primarily with Black communities — I worked in community health for years in Toronto before I joined the university in 2021. Black people have not had a history of good experiences with researchers or with academic institutions.
I want to see scientists integrate the ethical concept of protecting communities in their work, especially Black communities. We all need to hold researchers accountable in how they respect or disrespect Black communities.
This is where equity becomes crucial.
Equity in science means looking at access to data. The Black community has often been studied, but has lacked control of collected data and data analysis. It also means research focused on Black people, guided by their needs. And, it requires more Black researchers.
In 2016, a Statistics Canada census found that Black researchers made up 1.9 per cent of all full-time faculty in Canada, even though Black people comprised 3.5 per cent of the general population. (By 2021, that figure had grown to 4.3 per cent of the population.)
Notisha Massaquoi is the founding director of The Black Health Equity Lab. She is an assistant professor in the Department of Health and Society at U of T’s Scarborough campus, with a cross appointment to Temerty Medicine’s Department of Family and Community Medicine.
It drives inclusive research
My lived experience helps inform my work in medicine.
I’m in a unique position as an Indigenous physician who works with often underserved populations. I see equity from my individual lens as a Métis provider and from the lens of patients sometimes excluded from the conversation in health care and research. We still see racism and discrimination in health care. And, it happens to both patients and health care providers.
I remember being in medical school and self-identifying as Indigenous and people saying, “You must not have had to meet the same criteria because you are Indigenous.” But I had finished at the top of my undergraduate class, and then worked for seven years in public health. Just because of my identity, I was discounted and seen as an “equity hire.”
In the age of reconciliation, we need to include Indigenous communities in science, research, medicine and guideline development. It’s something we have never done well. Exclusion, racism and colonization have led to poorer health outcomes for Indigenous peoples, compared with the general population. We need to change this.
Similarly, people who use substances have faced a lot of stigma within the health care system. There is limited research on this population. Often, people who use substances are actively excluded from research studies, despite coming from every socio-economic and racial group. They span the nation, yet we have cut ourselves off from identifying ways to better care for them.
Equity means inviting and including all underserved populations into the conversation, informing what questions need to be answered and what research gets done. As we centre the patient voice more in research, we’ll see better outcomes, because we’ll have evidence-based medicine that works for all of the populations we serve.
Joel Voth (PGME ’23) is an addictions medicine physician and a member of the Indigenous Leadership Circle in Temerty Medicine’s Department of Family and Community Medicine.
What We Do for Others
Araz Sarchami
By Emma Jones
From the time he was a young boy, Araz Sarchami (MaSc ’07, PhD ’10) showed an immense aptitude for science and engineering.
“Growing up, Araz was so into creating stuff and making things,” says Araz’s sister Anna Sarchami. “He was always into playing with mechanical things like cars and toys. He would rewire them or take parts from one toy and get it to work on another.”
In 2021, Araz passed away unexpectedly in his sleep while visiting family in Iran. He was only 38 years old. The loss, Anna explains, was profound. Not only was Araz always keen to entertain his family — creating fabulous games and showing them new items to play with — but he was also dedicated to those around him.
“He believed everyone had their own special abilities. And, he helped them to achieve their goals as much as he could,” Anna says.
After completing his undergraduate degree in mechanical engineering at the University of Tehran in 2005, Araz completed both a master’s degree and PhD in the same area at the University of Toronto.
Nasser Ashgriz, a professor of mechanical and industrial engineering at the University of Toronto, supervised Araz’s master’s and PhD research in thermal hydraulics.
“He had the character of a true leader,” says Ashgriz. “It’s amazing how fast he would understand problems and find solutions. People were always coming to him for advice, and he was very eager to help them.”
After finishing his PhD, Araz quickly moved to bring his research to the world. In 2013, he became a co-founder of Coraltec, a company that developed a novel device for spray and particle characterization, based on his PhD research.
Araz had a willingness to share the results of his research with the academic community, presenting his work and submitting the results of his research at academic conferences. He also worked as an adjunct professor at U of T’s Faculty of Applied Science & Engineering, where he taught courses to both graduate and undergraduate students and worked as a mentor at U of T’s Entrepreneurship Hatchery.
Aziz Sarchami, Araz’s father and himself a graduate in mechanical engineering from the University of Tehran, remembers Araz would often speak to him about how phenomena seen in fluid dynamics could also be applied to blood flow in hearts supported by artificial ventricles.
“His mind was very open,” Aziz recalls. “He was thinking about how to connect mechanical engineering and medical research.”
But, in 2021, Araz tragically passed away. He had shown no signs of illness in the days and weeks leading up to his passing, making the news of his death both sudden and deeply shocking. His family was heartbroken. Friends and family who gathered to mourn Araz’s passing recalled how, on top of his passion for science, Araz was driven by a mission to help others.
In 2024, to honour their son, Aziz Sarchami and Giti Seyed Sadrimianji made a generous gift to establish the endowed Dr. Araz Sarchami Research Scholarship. Awarded to Temerty Faculty of Medicine graduate students focused on paediatric research, this gift will honour Araz’s memory by paying tribute to his dedication to uplift those around him.
After establishing the first award in Araz’s honour, Aziz Sarchami says they were inspired by Temerty Medicine’s research mission to improve medicine not just in Canada, but worldwide. Therefore, the pair soon established a second award, the endowed Dr. Araz Sarchami Doctoral Research Award, supporting researchers at Temerty Medicine’s Terrence Donnelly Centre for Cellular & Biomolecular Research.
University of Toronto’s Donnelly Centre is a global research hub which brings together world experts and researchers from a range of disciplines to foster a deeper understanding of the genome and its application in health.
This award, a nod to Araz’s interest in the connection between medicine and engineering, supports scientists and engineers advancing new understanding of the cellular and biomolecular underpinnings of life and its translation into life-saving solutions.
Aziz explains he finds comfort in the professors, researchers and students working together at U of T. The support they have for each other is what will drive new breakthroughs – reflecting the values Araz lived by.
“Years will go, and we will all pass away,” Aziz says. “But the things we do for each other will remain.” •
Celebrating Impact
Our Temerty Medicine alumni network consists of more than 71,000 health care leaders that includes graduates of our health sciences, rehabilitation sciences, radiation sciences, Physician Assistant, MD and MD/PhD programs, as well as former residents and fellows.
Each year, the Dean’s Alumni Awards celebrate and highlight alumni who have made extraordinary contributions to the advancement of health and health care. Congratulations to this year’s honourees!
Learn more about the Dean’s Alumni Award recipients and other alumni programs.
Rob Fowler (PGME ’98 & ’99 Internal Medicine)
Humanitarian Award
Humanitarian Award
Rob Fowler is the H. Barrie Fairley Professor of Medicine and director of the Interdepartmental Division of Critical Care Medicine at U of T, and chief of the Tory Trauma Program at Sunnybrook Health Sciences Centre. In both his research and practice, he focuses on improving access to and outcomes of care for critically ill patients worldwide. A global leader in outbreak response, he has supported the World Health Organization and other non-governmental organizations during viral hemorrhagic fever outbreaks across Africa. His volunteer service — often at great risk to his own health — has earned him numerous awards, including the Meritorious Service Cross, Order of Ontario, and the Teasdale-Corti Humanitarian Award.
Peter Gill (PGME ’18 Paediatrics)
Emerging Leader Award
Emerging Leader Award
Peter Gill is a general paediatrician and scientist at the SickKids Research Institute, an associate professor of paediatrics and of health policy, management and evaluation at U of T, and a senior associate at the Centre for Evidence-Based Medicine at the University of Oxford. He co-founded and is chair of the Canadian Paediatric Inpatient Research Network (PIRN), uniting hospitals nationwide to improve care for hospitalized children. His research has advanced the care and management of common and serious childhood infections and has earned him national recognition, including the Canadian Paediatric Society Young Investigator Award and the Paediatric Chairs of Canada Emerging Academic Leader Award.
Tara Kiran (MD ’02)
MAA MD Alumni of Distinction Award
MAA MD Alumni of Distinction Award
Tara Kiran is the Fidani Chair in Improvement and Innovation at U of T and vice-chair of quality and innovation with the Department of Family and Community Medicine. A family physician and renowned primary care researcher at Unity Health Toronto’s St. Michael’s Hospital, Kiran investigates how changes in the health care system impact patients, particularly the most vulnerable. In 2022 she launched OurCare, a national initiative to engage the public in co-creating the blueprint for a stronger, more equitable primary care system in Canada. She is also the creator and host of Primary Focus, a podcast that shares stories and innovations from Canada and around the world to inspire a stronger primary care system.
Gareth Seaward’s commitment to excellence in clinical practice and medical education have left an enduring legacy in obstetrics and gynaecology in Canada, as evidenced by the enthusiastic nomination support from his hospital and Institute of Health Policy, Management and Evaluation colleagues. Seaward is a professor of obstetrics and gynaecology and of health policy, management and evaluation at U of T, as well as a distinguished obstetrician-gynaecologist and a globally recognized pioneer in maternal-fetal medicine. He served as the deputy director of the fetal medicine unit at Sinai Health’s Mount Sinai Hospital for 20 years. He also held leadership roles at the Provincial Council for Maternal Child Health for over a decade, where he supported the development of recommendations, tools and guidelines that continue to help health care professionals across Ontario provide high-quality and effective perinatal care.
Steffanie Strathdee (PhD ’94 Epidemiology)
Impact Award
Impact Award
Steffanie Strathdee is the Harold Simon Distinguished Professor at University of California San Diego and co-founder and co-director of the Center for Innovative Phage Applications and Therapeutics, the first of its kind in North America. She earned her PhD in 1994 from the Department of Community Health within U of T’s Faculty of Medicine (now the Temerty Faculty of Medicine). The department became the Dalla Lana School of Public Health in 2008. A renowned infectious disease epidemiologist, she has led groundbreaking work in HIV prevention and antimicrobial resistance. Her efforts to revitalize phage therapy in the West earned her a place among TIME’s 50 Most Influential People in Health Care in 2018.
Illustration by Jud Haynes
By Blake Eligh
Family doctors are the first point of contact for many patients, yet family physicians face mounting pressures: heavy workloads, growing administrative tasks and long hours that fuel rising rates of burnout and contribute to a shortage projected to leave more than four million Ontarians without a primary care physician by 2026.
At Women’s College Hospital’s Institute for Health System Solutions and Virtual Care (WIHV), Onil Bhattacharyya (PhD ’07) is working to ease those pressures by embedding research directly into care. Bhattacharyya, the Frigon Blau Chair in Family Medicine Research and WIHV’s director, says the institute is a place to test new technologies in simulation and real clinics, refine them with feedback from family physicians and then use that evidence to inform product developers and policymakers.
“We offer clinics the opportunity to test and give feedback on technology that could be deployed across the province,” says Bhattacharyya, an associate professor in the Temerty Faculty of Medicine’s Department of Family and Community Medicine. “It’s a platform to evaluate combinations of tools and see how they can advance primary care.”
A major focus has been the evaluation of AI scribes — software that generates clinical notes during patient visits. With more than one-third of family physicians reporting burnout, much of it tied to paperwork, the promise of this technology has drawn enormous interest. In 2023, WIHV began with controlled studies, pairing doctors with simulated patients before piloting AI scribes with 150 family doctors and nurse practitioners.
The results of the three-month pilot were encouraging: Respondents reported saving up to four hours of after-hours administrative work weekly, with 70 per cent less time on clinical documentation, and experiencing reduced stress with more time for patient care. The data supported adding AI scribes to provincial procurement systems for broader trials. Rolled out in Ontario and other provinces across Canada, more than 10,000 physicians signed up in just two weeks, representing about 20 per cent of Canadian family doctors.
The suite of studies is among the first to systematically evaluate the usability, effectiveness and accuracy of AI scribes in primary care. Bhattacharyya and his WIHV colleagues are now studying how the tool works at scale, including the impact of AI on documentation quality. For Bhattacharyya, the value lies as much in the research model as the technology. By involving family doctors in evaluation, WIHV ensures vendors refine the products to meet real needs, while policymakers gain the evidence required to make procurement decisions.
“There’s enormous appetite for this information,” he says. “Ontario’s Ministry of Health has to make hard decisions without a lot of data. Our work helps to fill those gaps.”
WIHV’s interdisciplinary team of researchers includes Enid Montague, a professor of industrial engineering in U of T’s Faculty of Applied Science & Engineering. She says collaboration between engineers and physicians is essential to ensure AI improves, rather than complicates, patient care.
“When engineers and physicians collaborate, we can apply systems analysis, workflow design and human-centred evaluation to ensure technologies truly support clinicians,” she says.
“By learning from each other, we’re designing AI systems that enhance performance and preserve the human connection.”
Montague says one of the most striking outcomes came during the simulation phase of the study.
“I was excited to see joy return to the process. Physicians got to listen,” she says. “They weren’t typing or trying to hold on to so much information. I got to witness people enjoying being doctors again. That’s something we don’t always expect from AI.”
Bhattacharyya notes that collecting data from family physicians, many of whom work in independent clinics, is more challenging than conducting studies in large hospitals.
“This work gives voice to family doctors,” he says. “They’re directly involved in testing products and providing feedback to vendors, procurement and policymakers.”
Beyond AI scribes, Bhattacharyya and provincial co-leads are also evaluating Health 811, an online tool that offers patients 24-7 access to symptom checkers, education and connections to care. He is working with Health 811 leads from every province and territory to create a community of practice to support strategic decisions and turn Health 811 into a digital front door for health care systems. Bhattacharyya’s work keeps him close to both physicians and policymakers, and he says WIHV shows how applied research can drive change across the health care system.
“As a scientist, it’s great to figure out what matters, to have a finger on the pulse of what decisions are being made and have the opportunity to be engaged in the process,” he says. •
Photo of Ahmed El-Sohemy
By Heather McCall
Sitting in a quiet university lab back in 1994, Ahmed El-Sohemy (PhD ’99) was perplexed.
He had recently started his master’s degree in nutritional sciences at the University of Toronto’s Faculty of Medicine — now the Temerty Faculty of Medicine — and was conducting a routine experiment to test the effects of cholesterol on cancer development in female rats.
The results, however, were anything but ordinary to El-Sohemy. What he observed — a difference in mammary tumour development linked to how the rats responded to dietary cholesterol — differed from the findings of earlier studies by other researchers.
Certain that he must have made a mistake, El-Sohemy painstakingly retraced his steps, confirming every detail of his method. The only factor he could surmise that might explain the discrepancy? The strain, and thus the genetic makeup, of the animal subjects themselves.
It was a lightbulb moment — one that led to later research by El-Sohemy examining if animals’ diets and genetic makeup influence their incidence of cancer.
“If two rats can respond differently to cholesterol, then surely two humans can respond differently — not just to cholesterol, but to anything,” El-Sohemy thought.
These insights would become the foundation of his postgraduate research and the eventual cornerstone of his career, sparking a lifelong pursuit to understand how genetic differences may shape human responses to nutrition. The results of El-Sohemy’s experiments may also explain why nutritional science research can yield contradictory findings, he says.
“Take coffee, for example,” he says. “One day we hear it’s good for us, another day we hear it’s bad. Our findings suggested it could be possible for coffee to be good for one person, yet harmful for somebody else.”
Trying to puzzle out why things operate the way they do has always fascinated El-Sohemy, who has long been driven by a personal interest in sports and performance.
This interest is why he channelled his energy into an undergraduate degree in nutritional sciences, imagining that he would ultimately study sports medicine. However, a summer research project in 1993 that was initially intended to bolster his medical school application changed everything.
“I realized that through research I could do something that nobody in the world had ever done,” he says.
Captivated by the scientific process, he bypassed medical school entirely and dove headlong into graduate studies at U of T, eventually reclassifying from a master’s to a PhD program in nutritional sciences. After witnessing how genetic variations could explain conflicting results in animal studies, El-Sohemy set his sights on expanding the scope of his research.
He pursued a postdoctoral fellowship at Harvard University, one of the few places exploring the intersection of human nutrition and genetics in the emerging field of nutrigenomics. Specifically, he wanted to better understand how genes influence individual responses to nutrients and food bio-actives, such as caffeine.
He then returned to U of T in 2000, accepting a faculty position as an assistant professor in Temerty Medicine’s Department of Nutritional Sciences. From 2003 to 2013, El-Sohemy held a Tier 2 Canada Research Chair in Nutrigenomics, co-authoring studies that linked genetic variations to vitamin metabolism, sugar cravings and nutrient absorption.
Rather than focusing on averages, the studies examined people who were outliers — individuals who responded unusually well or poorly to dietary interventions — and traced those differences to genetic markers.
“Most of our research program was based on revisiting just about everything we thought we knew about nutrition,” he said. Since then, the connection between genetic variations in caffeine metabolism has been seen in studies linking caffeine intake with hypertension, kidney disease and the risk of prediabetes.
In 2011, El-Sohemy set his sights on translating his research into a consumer product — a genetic testing service that could offer people a personalized nutrition profile. He founded Nutrigenomix Inc. as a U of T startup and officially launched it in 2012. To ensure the results are correctly interpreted, the service is for health care professionals acting on behalf of their clients. These practitioners then use the data provided by El-Sohemy’s company to tailor meal plans and nutritional advice based on each client’s genetic profile.
“For me, credibility and my reputation as a scientist come before any profit,” he said. “That’s why we’ve also invested considerably in supporting research.”
Nutrigenomix is now in 95 countries and includes more than 13,000 dietitians and other health care professionals who use the service to advise their patients. Looking ahead, El-Sohemy sees vast potential for personalized nutrition.
“If you eat and drink, and you care about your health, you’re a good candidate for testing,” he says. •
Preparing for emergencies
By Gabrielle Giroday
How do you train emergency medicine residents to treat an influx of 30 patients after a toxic chemical spill?
Or, how to care for a patient who’s about to give birth in the emergency room?
What if they need to try to save someone who’s had a heart attack after experiencing hypothermia?
As the simulation lead, Amit Chopra (MD ’20, MSc ’16) is helping residents in the Temerty Faculty of Medicine’s Emergency Medicine program train for these types of scenarios. These practice sessions intentionally copy real-life medical cases known as HALO procedures, or “High Acuity, Low Occurrence” (HALO) situations.
HALO procedures are not routine, everyday medical events. They are life-threatening cases that doctors may see occasionally in an emergency department, which means it’s especially important for residents to practise how to handle them in advance of them happening.
“In emergency medicine, we have to be prepared for the unexpected. We don’t necessarily have to master each area in medicine, but we have to be able to manage the initial five to 10 minutes of care for any patient who needs our help,’” he says.
Chopra and Kaif Pardhan (PGME ’15), the director of Temerty Medicine’s Emergency Medicine residency program, are in charge of the in-person simulations for the 56 residents currently in the five-year program. The program builds the residents’ ability to work in teams, as they will in an emergency department. This means medical professionals must invest in sharpening their skills in areas such as communication and role allocation, he says.
“We know that training for the unexpected as a team in a controlled setting prepares you to work together more effectively in time-sensitive and high-pressure situations,” he says.
The HALO simulations, which are led by instructors, can feature mannequins or actors portraying patients, and usually last about one hour. The simulations can follow two formats.
The “in situ” format takes place in an emergency department in a hospital with emergency department staff, including physicians, nurses, clerks and other health care providers. Here, the whole team has the opportunity to practise treating a specific case together and then examine how they can improve for the future.
The other format takes place in a specialized simulation centre located at Unity Health Toronto’s Li Ka Shing Knowledge Institute and features only residents. Training in both types of formats means better overall teamwork between health care professionals when HALO cases do happen, and better patient outcomes overall.
For example, Chopra points to research that shows simulations can improve outcomes for bleeding trauma patients and enhance residents’ speed and comfort in performing airway openings called cricothyroidotomies.
“In the emergency department, we’re working with a different set of people on every shift, and there may be types of medical cases that we see only once or twice a year — or less frequently,” says Chopra. “If we have trained to work collaboratively in diverse teams, the patient outcomes tend to be much better, not only because the medical professionals are more comfortable working together, but because we’re ready for any unexpected problems that can arise.” •
Photo of Jennifer Doudna, taken by Erin Howe
A Nobel laureate on the future of science
Standing up for science means championing curiosity and diverse perspectives, says Jennifer Doudna, a professor in the Departments of Chemistry and Molecular and Cell Biology at the University of California, Berkeley, and founder of the Innovative Genomics Institute.
Doudna knows about big breakthroughs — she received the 2020 Nobel Prize in Chemistry, alongside Emmanuelle Charpentier, for the pair’s discovery and development of CRISPR-Cas9 as a genome editing tool.
Writer Betty Zou (PhD ’15) spoke with Doudna, who holds the Li Ka Shing Chancellor’s Chair in Biomedical and Health Sciences, before she delivered the Temerty Faculty of Medicine’s 2025 Oliver Smithies Lecture in October.
What does standing up for science mean to you?
I think science is such an incredible opportunity for human beings to try and understand our world. It’s been an amazing engine of discovery and progress — economic, technical, medical, environmental. I think it’s important to embrace that and to think about what we can do now to encourage more people to be interested and engaged in science going forward.
What is the value of fundamental, curiosity-driven science?
The thing about science is that we don’t know where it’s going. If we want to make new discoveries and real breakthroughs, that requires a willingness to explore the unexplored, to try things that have never been tried before, to have a wild idea and be willing to pursue it. That’s where we need governments and non-profit organizations to step up and to be willing to put money into that kind of discovery. We need to have a very active base of fundamental research that drives the enterprise that’s critical for the future of science and for humanity.
You’ve been a long-time advocate for diversity in science. Why is that important to you?
When I started my career, I had no idea how valuable it is to have different people with different cultural backgrounds, points of view, ideas, interests, and passions, all converging in a research lab to study a problem or work on a particular project. It’s the idea that you’re not likely to make breakthroughs if everybody is thinking the same way.
What do you see as the role of the University of Toronto in this current moment?
The University of Toronto, for me, has always stood for wonderful fundamental research that translates into real applications, especially in human health. I think that really does give U of T a platform for stepping up and speaking up for the value of science in a positive way — just really focusing on what we do, why we do it, why it’s valuable, why it’s useful, why it’s interesting, why it’s exciting. •
This interview has been edited for length and clarity.