We flinch in anticipation — a squint, a grimace, a breath held tight.
Sudden or slow. Lingering or fleeting.
Pain is the body’s Red Alert — shaping how we move, live and heal.
More than sensation, pain is a memory, biology, psychology.
The stories in this issue trace the edges of pain — how we feel it, fight it and begin to understand it.
And how science is moving us closer to lasting relief.
Once dismissed as invisible and untreatable, medicine is finally taking chronic pain seriously — and a new kind of care is taking shape.
By Scott Fotheringham
Half a lifetime ago, Vina Mohabir was a straight-A student with a busy life filled with clubs, extracurriculars, friends and family. That all changed after a 2010 accident left the teenager with head trauma and facial injuries, triggering trigeminal neuropathy and chronic migraines.
At just 15, the teen was in constant pain and deeply isolated. The idea of a future in that state felt unbearable, and she often thought of suicide.
“I had pain that just wouldn’t go away after the ‘normal’ amount of time of healing,” Mohabir recalls.
“It completely changed my life,” she continues. “Because my pain was invisible, it was hard for people to understand how it influenced every part of my life. I often heard, as a girl, that I was dramatic or attention-seeking.”
A Public Health Priority
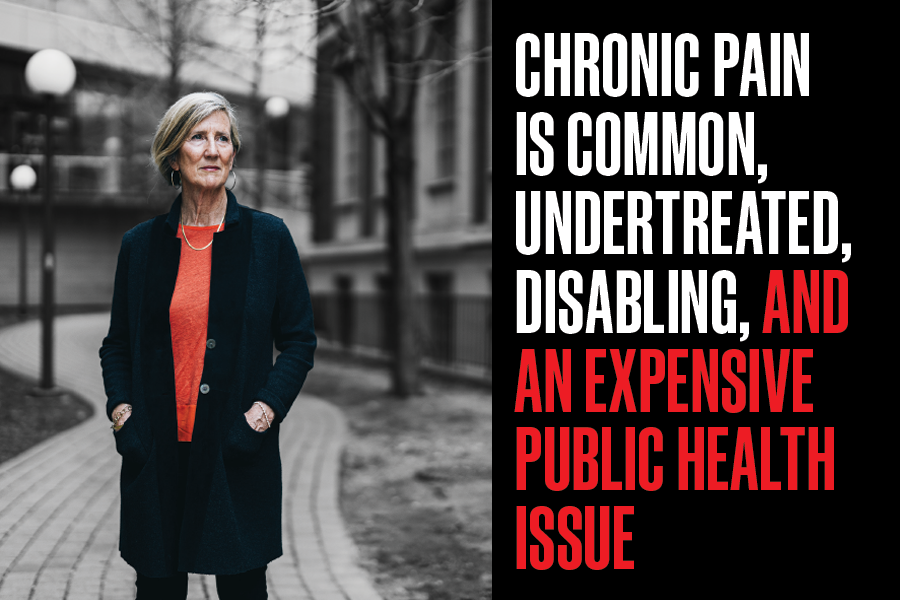
Mohabir is one of the estimated eight million people in Canada who struggle with chronic pain (lasting longer than three months).
Beyond the economic impact of chronic pain on health care and productivity — estimated at up to $40.3 billion a year in Canada — persistent pain affects work, education and relationships, and often comes with mental and physical health issues. It can be poorly managed — especially in childhood — leading to long-term health impacts.
It was the opioid crisis that prompted governments to tackle chronic pain more seriously. In 2019 the federal government launched the Canadian Pain Task Force to better understand and address the issue, leading to Health Canada’s Action Plan for Pain in Canada in 2021.
“Chronic pain is undertreated, disabling and an expensive public health issue,” says Fiona Campbell (PGME ’91) co-chair of the task force and co-director of the Pain Management, Research and Education Centre (Pain Centre) at The Hospital for Sick Children (SickKids). “It disproportionately affects equity-deserving populations — those who are gender diverse, living in poverty, racialized, Indigenous, newcomers and women.”
Also in 2019, the World Health Organization reclassified chronic pain as a disease, bringing pain into the spotlight to help reduce stigma and drive research.
Campbell’s work with the task force led to the creation of a chronic pain policy team at Health Canada and funding for Pain Canada, a national non-profit unifying provincial care strategies.
She held the inaugural chair of the Ontario Chronic Pain Network, which, in partnership with the provincial health ministry, is now exploring low-cost, community-based care to reduce reliance on tertiary care.
“Tertiary care clinics serve those with the most severe impact on quality of life,” says Campbell, who is also a professor and the director of the Chronic Pain Management Program at the Temerty Faculty of Medicine.
“But with chronic pain affecting one in five people, we’re never going to be able to see all those affected. We need accessible care along the continuum, from community supports to specialist services.”
The Science Behind Chronic Pain
While the public health conversation focuses on care systems, researchers are working to understand why chronic pain happens in the first place and why it’s so hard to treat.
Acute pain is protective and normal; it’s the body warning of imminent tissue damage. The processing of a damaging stimulus — burning your finger, for example — results in the subjective experience of pain, known as nociception.
“Pain starts in the periphery, where primary sensory neurons detect a stimulus,” says Steven Prescott, a senior scientist at SickKids and physiology professor at Temerty Medicine. “The signal travels to the spinal cord, then into the brain’s cortex, where more processing occurs.”
But in chronic pain, the warning system breaks down. Signals may misfire, even without tissue damage.
“Chronic pain seems to be the inter-action of changes in the brain and the periphery,” Prescott says. “It might be caused by chronic inflammation or injury that causes a cascade of changes and makes nociceptors or other types of neurons hyperexcitable and hyper-responsive.”
When the signals are mixed up, a light touch can be excruciating.
Research to Yield New Treatments
As an MD/PhD student, Prescott was frustrated by treatment limitations and turned to basic research.
“We need to step back and ask fundamental questions about how pain is coded by the nervous system if we want to produce effective treatments,” he says.
Prescott has seen this firsthand in studies of a specific sodium channel found only in pain receptors. Drug-makers hoped blocking the channel would relieve pain without widespread side effects, but clinical trials fell short.
“People hoped that if we blocked one sodium channel, everything would go back to normal,” says Prescott. “But we’re dealing with a half-dozen sodium channels, potassium channels, synaptic and inhibitory receptors. It’s difficult to tease apart primary and compensatory changes.”
Prescott outlines two ways to treat chronic pain with drugs. The first is to correct what has changed to cause pathological pain. Most of these discoveries are serendipitous — the drugs work, but not for the reasons we initially thought. For example, gabapentin, used to treat nerve pain from shingles and other diseases, was designed to mimic gamma-aminobutyric but acts on calcium channels instead.
“The other method is to intervene with the body’s natural pain control mechanisms,” Prescott says. “This includes opioids, which engage endogenous pain control systems. As well, there’s spinal cord stimulation, which uses electrical stimulation to activate inhibitory neurons to control pain.”
The Plasticity of the Nervous System
Min Zhuo, a physiology professor at Temerty Medicine, believes chronic pain should be thought of as a brain disease, not a localized injury issue.
His research shows how central nervous system (CNS) plasticity alters pain perception and complicates drug discovery. In 2001, Zhuo’s lab was the first to show that digit amputation can cause long-term potentiation (LTP) in the anterior cingulate cortex (ACC) neurons of adult rats. LTP is the brain’s way of reinforcing connections between nerve cells so they can send signals more effectively.
“We’ve made major progress showing that acute pain is different from chronic pain in basic mechanisms and molecular targets,” Zhuo says.
“For years, scientists believed targeting pain directly would work, but multiple preclinical drug tests failed because of central plasticity, mainly LTP, in the pain pathway, including the cortex.”
In LTP, synaptic connections strengthen with recurring stimulation, leading to chronic pain by amplifying signals after the original stimulus ends.
“The rapid plasticity of the CNS causes neural networks to be more readily activated by peripheral sensory stimuli,” says Zhuo. “This can lead to hyperalgesia, when the same pain stimuli cause more pain, or allodynia, when a gentle touch can become painful.
“LTP may trigger new gene and protein expression and contribute to cortical reorganization, which has been demonstrated in patients with phantom pain.”
Better Methods to Measure Pain
Conventional pain assessment relies on observing behaviour, such as motor responses. Zhuo advocates for supplementing this with direct measurements of neuronal plasticity, including gene activation and protein changes in the ACC.
“Most drug discovery relies on animal behaviours to evaluate the potential effects of drugs,” Zhuo says. “However, behavioural responses are influenced by many factors.”
Cortical LTP provides a more objective measure. He says that monitoring both synaptic and neuronal network activity offers a clearer picture of chronic pain’s physical and emotional components.
“Chronic pain is rarely ‘pure’ pain,” says Zhuo. “It’s usually the integration of pain, emotions and stress. Optogenetic methods, which use light to control the activity of neurons and cells, are helping us gain insight into the network and individual synapse plasticity in chronic pain. Better behavioural measurements, combined with in vivo recording and imaging, will help our understanding of chronic pain.”
Treating the Whole Person
Chronic pain is rarely eliminated, but with support, people living with pain can still lead rich, meaningful lives. That journey begins with a holistic approach.
Brain imaging studies reveal that the regions responsible for physical pain and emotion overlap, which is why emotional interventions can help ease pain.
At SickKids, the team follows a “3Ps approach”: pharmacotherapy, psychological therapy and physical strategies to improve function, lower stress and build coping skills.
“It’s important that people know that seeing a psychologist doesn’t mean we believe chronic pain is all in a patient’s head,” says Campbell. “We’re helping them to use their powerful brains to dial down pain.”
Clinicians should view chronic pain through a biopsychosocial lens, Campbell says. For example, physical therapists might work with patients on function and building confidence in movement, while psychological supports address fears that activity may cause or worsen pain.
“Pain is personal,” says Jennifer Stinson, a senior scientist with SickKids’ Child Health Evaluative Sciences program and a professor at the University of Toronto’s Lawrence S. Bloomberg Faculty of Nursing. “The goal is to help people live better lives, even if we can’t eliminate pain entirely.”
Coming Full Circle
It’s something Mohabir knows firsthand. As a teen, she was treated at the SickKids Pain Centre by an integrated care team that included Campbell, Stinson, as well as a psychologist, physiotherapist and occupational therapist.
“The Pain Centre gave me the skills to manage the chronic condition I’ll have for the rest of my life,” she says.
Today, Mohabir works with the Pain Centre as a patient partner while pursuing her doctorate at U of T’s Institute of Health Policy, Management and Evaluation in Stinson’s iOUCH Pain Lab.
Her research focuses on using digital tools, such as the iCanCope platform, which she helped develop as a patient partner, to reduce stigma for youth with sickle cell disease.
Mohabir wants pain care integrated more fully into routine health care systems — from surgical followup to youth mental health to family medicine — and for patients to help co-design that care.
“My hope is to use one of the worst experiences of my life to empower others,” Mohabir says. “In another 15 years, I hope you can talk to someone whose outcomes were even better than mine.” •
Illustration By Jud Haynes
Reimagining Pain Management
By Betty Zou
As a teenager, Andrea Furlan suffered severe menstrual cramps. “Nothing worked for my pain, so I had to miss a lot of school and other activities,” she recalls. Those early experiences helped shape her future in medicine.
Today, Furlan (PhD ’06) is a professor of physical and rehabilitation medicine in the Department of Medicine at the Temerty Faculty of Medicine. She’s part of a growing movement of clinicians and researchers reimagining how pain is understood — and how it might be treated differently. Driven by a shared mission, they’re laying the foundation for more personalized, patient-centred pain care.
One Size Doesn’t Fit All
“We use a fairly broad-stroke approach to treating pain, but not all pain is the same,” says Rachel Tyndale (MSc ’88 & PhD ’91), a senior scientist at the Centre for Addiction and Mental Health (CAMH), and a professor of psychiatry, and pharmacology and toxicology at Temerty Medicine.
She envisions a future in which treatment is tailored to an individual’s biology. “We’re at the very early stages of creating treatments paired to each type of pain and knowing when they’re going to work for different people.”
For now, researchers are making the most of the drugs that they do have to treat pain more safely and effectively.
“What we often do in pain management is repurpose drugs like antidepressants or anti-seizure medications,” says Karim Ladha, the Evelyn Bateman Recipe Chair in Ambulatory Anesthesia and Women’s Health at Women’s College Hospital.
Ketamine is one such example. Originally approved as a general anesthetic, low doses have since shown promise in treating chronic pain conditions and treatment-resistant depression.
Searching for Alternatives
Ladha’s patients and their evolving attitudes toward pain medicine shape his research. “People today are very hesitant to take opioids,” says Ladha, a clinician-scientist. “Patients really want an alternative, and we’re trying to find one for them.”
In the search for non-opioid alternatives, Ladha and colleagues are leading clinical studies to better understand the effects of cannabis on chronic pain. Their goal: to identify which patients are most likely to benefit and which cannabis compounds offer the most effective pain relief.
Ladha is also leading a new randomized clinical trial to examine whether psilocybin, the active ingredient in magic mushrooms, can alleviate chronic neuropathic pain, a debilitating condition characterized by constant shooting, burning or stabbing sensations.
Even though some of these drugs have been used for a long time, Ladha stresses the importance of rigorous research to evaluate safety and effectiveness. The spectre of the opioid epidemic — and the deceptive marketing that led to it — looms large.
“When you look at the marketing around opioids, people consistently said it was safe. And when you listen to people speak about cannabis or psychedelics now, they are using some of the same language,” says Ladha, who is also an associate professor in Temerty Medicine’s Department of Anesthesiology and Pain Medicine.
“We want to be very cautious not to make those same mistakes again.”
Tailoring Treatment Through Genetics
While these new treatment options herald the possibility of an opioid-free future for some, there will always be a subset of patients whose pain is best managed with opioids. The question is how to minimize harm while maximizing benefit.
The answer could lie in our genes.
Over the past 15 years, researchers have identified genetic variations associated with an increased risk of developing opioid use disorder or experiencing opioid-induced adverse events such as respiratory depression, a potentially fatal side effect marked by slow, shallow, irregular breathing. Because of these genetic differences, two people given the same dose of an opioid can have drastically different responses that, in turn, can lead to varied levels of pain relief and risk.
As the Canada Research Chair in Pharmacogenomics, Tyndale has studied how genetic factors could influence the response to methadone and buprenorphine/naloxone, two medications used to treat opioid use disorder. In a 2023 study she co-led with Bernard Le Foll, a CAMH senior scientist, Temerty Medicine professor of family and community medicine, pharmacology and psychiatry, and the chair of addiction psychiatry within the Department of Psychiatry. The researchers identified a specific variant in an opioid receptor gene linked to poorer outcomes with methadone.
Tyndale says, “It suggests that there may be predictable genetic differences between people in how well they respond to methadone as a treatment drug.”
She sees pharmacogenetics as a tool that could eventually help clinicians select the medication most likely to work and be safe for each patient, whether it’s to manage pain or treat opioid use disorder.
Biomarkers in the Brain
What if biomarkers could help assess a person’s risk of developing opioid use disorder?
At CAMH’s Brain Imaging Centre, Le Foll collaborates with associate director, Isabelle Boileau, a Temerty Medicine professor of psychiatry, and pharmacology and toxicology. They conducted a first-of-its-kind study examining the association between the fatty acid amide hydrolase (FAAH) enzyme and opioid use disorder in the brains of living individuals.
FAAH is part of the body’s endocannabinoid system, which controls important functions such as learning, memory and pain. In animal models and human case studies, low levels of FAAH have been linked to a reduced ability to feel pain; however, the exact mechanisms of this linkage are unknown.
To better understand the role of the enzyme in pain and addiction, CAMH researchers developed the world’s first positron emission tomography (PET) imaging tracer to directly measure FAAH activity in the brain. Their earlier work established a link between lower enzyme activity and a higher risk of alcohol and cannabis use disorders.
“We wanted to know if FAAH is also a biomarker for opioid use disorder,” says Claire Shyu, a doctoral student in Temerty Medicine’s Department of Pharmacology and Toxicology, who is leading the project.
In the pilot study, the researchers recruited two groups of people living with chronic pain and regularly taking prescription opioids; one group had a history of opioid use disorder, the control group had no such diagnosis. The team is now analyzing the data to determine whether differences in brain FAAH activity levels exist between the two groups, potentially providing new insights into the enzyme’s role in sensing pain and in addiction-related behaviours.
Better Prescribing
For people at high risk of developing opioid use disorder or severe side effects, such as sleep apnea, the decision to reduce opioid use may be a difficult but necessary decision.
“It’s 10 times harder to taper a patient off opioids than to start them,” says Furlan, who is also a senior scientist at University Health Network’s Toronto Rehabilitation Institute.
Despite the central role that family physicians play in managing chronic pain, few are trained in how to support patients through opioid tapering. In a 2010 cross-Canada survey that Furlan and colleagues conducted, shortly before the release of the first Canadian opioid guideline, the respondents revealed substantial gaps in knowledge and practice in how to discontinue opioid use. A followup survey in 2018 found that while physician attitudes toward opioids had improved, significant knowledge gaps still persisted.
To help close those gaps, Furlan created an accredited online course focused on managing chronic non-cancer pain. The course covers topics such as how to select and titrate opioid doses, and safe tapering strategies. Since its launch in 2019, over 2,800 opioid prescribers, learners and other stakeholders have taken the course.
Furlan also chairs ECHO Ontario’s Chronic Pain and Opioid Stewardship program, a telementoring project that teaches clinicians in rural and underserved areas how to best support patients with chronic pain. Weekly 90-minute sessions feature a case discussion followed by a topic-based presentation.
Furlan reports that many of the participants come away with more confidence and clearer strategies for helping patients to reduce their use of opioids or stop them altogether, and where to turn for guidance and resources.
Reaching for a Lifeline
One of the topics Furlan covers in her online course and ECHO sessions is the I-WOTCH study, a randomized clinical trial conducted in the United Kingdom that tested a novel approach to help people with chronic pain reduce their opioid use.
Participants were randomly assigned to receive either usual care — which included a self-help booklet on pain and opioids, and a relaxation CD — or a new intervention featuring a standardized opioid tapering plan, weekly group meetings, individual consultations and followup phone calls.
After 12 months, nearly 30 per cent of participants in the intervention group had stopped using opioids, compared to just 7 per cent in the usual care group. The results surprised even Furlan and her colleagues.
“Almost one in three people didn’t need opioids and were able to stop without making their pain worse,” says Furlan, who co-authored the study.
The participants who received tapering education and support also reported better secondary outcomes such as improved sleep, mental health and overall quality of life.
Despite the trial’s encouraging results, Furlan has been disappointed by the limited uptake of the new intervention. While the educational components are time-intensive, she thinks a bigger barrier may be that many physicians lack familiarity with opioid tapering. This is why she remains committed to reaching as many prescribers as possible through her online course and ECHO.
“We already have the tapering strategies,” she says. “But to do it right, both sides of the table — the patient and the prescriber — need to be motivated and know why they’re doing it and feel confident that they can follow through.” •
Professor James Khan
The Future of Preventative Pain
By Mark Witten
Most of us can expect pain after surgery or an injury. But for many, that acute pain doesn’t go away. Instead, it becomes chronic, affecting quality of life and straining the health care system.
For decades, chronic pain has been treated reactively, once it has taken hold. But now, researchers on the cutting edge of pain science are testing preventive treatments — such as lidocaine infusions, and even high-dose vitamin C — to stop pain from becoming chronic.
On the clinical front, networks of pain specialists are introducing early interventions to reduce suffering and reliance on opioids, and to help patients take control of their recovery.
A Study in Pain Prevention
Persistent pain after breast cancer surgery, known as post-mastectomy pain syndrome, offers a stark example of the limits of reactive care.
“About one in three women will suffer from chronic pain after a mastectomy or lumpectomy,” says James Khan, (PGME ’19) a professor and clinician-scientist at the Temerty Faculty of Medicine’s Department of Anesthesia and Pain Medicine.
“This is a staggeringly high rate of chronic pain after a surgical procedure,” he continues, adding that this debilitating complication is underrecognized and often missed in followup care.
“Unfortunately, patients who continue to have pain one year after surgery will likely suffer pain for the next 10 years or longer.”
Khan aims to break the cycle by targeting the pain pathways before operating. He is leading a large international trial at University Health Network to test whether intravenous lidocaine, given during surgery, might prevent and reduce the incidence of chronic pain after breast cancer surgery.
Lidocaine, a common local anesthetic, blocks sodium ion channels in nerve cells that transmit pain signals. The global trial aims to enroll 1,602 patients from 18 recruitment sites in Canada, Africa, Europe and South America.
“If our study proves lidocaine can help prevent chronic pain, it has the potential to be used routinely and be integrated as a standard of care globally,” says Khan, director of the Persistent Breast Cancer Pain Clinic at Mount Sinai Hospital.
Rewiring the Pain Pathway
Why does breast cancer surgery trigger persistent pain in some patients but not others?
The chest wall and breast tissue are dense with small peripheral nerves that can be damaged during surgery. When injured, they may undergo changes in sodium ion channels, increasing pain signals to the brain. This causes the brain to process pain signals faster and amplify sensations across the nervous system, like a radio stuck at high volume.
“These sodium ion channel changes may be temporary in some patients, but in others may lead to long-term pain,” says Khan. “Administering lidocaine before and during surgical resection may suppress these ion channel changes locally and centrally, effectively interrupting the process that leads to chronic pain for these patients.”
Screening Before the Scalpel
David Flamer (PGME ’15), a professor in Temerty Medicine’s Department of Anesthesia and Pain Medicine, leads Sinai Health’s Transitional Pain Service, which screens patients throughout the surgery process.
“We work with patients before, during and after their hospital stay to find the right treatment plan for their individual needs,” says Flamer, an anesthesiologist and the director of Pain Services at Sinai Health.
“This builds trust with the pain care team and empowers patients in their recovery,” he says. “It goes a long way toward minimizing the risks of persistent pain and overreliance on opioids.”
Sinai Health’s Enhanced Recovery After Surgery program is a collaborative initiative of the orthopaedic and anesthesia teams. Flamer and colleagues use targeted nerve blocks to reduce pain following a knee replacement, allowing patients to go home the same day with a wearable catheter that delivers continuous pain relief.
“We’re seeing better pain control and faster recovery,” Flamer says. “It’s exciting to implement new techniques and approaches. The more effectively we manage acute pain, the less likely it is to become chronic.”
The Immune System’s Surprising Role
Scientists are also looking deeper to uncover immune system responses that might determine whether pain lingers or fades.
At McGill University, Luda Diatchenko, professor of medicine and dentistry, and Canada Research Chair in Human Pain Genetics, studies how inflammation shapes pain outcomes.
In a study published in Science Translational Medicine in 2022, Diatchenkoand co-authors report that patients with lower back pain or temporomandibular disorder who had a strong early immune response were more likely to recover. Those who developed chronic pain showed a weaker initial inflammatory response and remained trapped in a state of low-grade inflammation that gradually increased over time.
Diatchenko’s research suggests that a balanced immune response, in which an initial acute inflammatory response triggers the body’s natural, dynamic immune healing process and subsequent resolution of inflammation, might protect individuals from chronic pain.
“We need a more nuanced pain management approach — one that can harness and activate the immune system, not inhibit it, so that treatment prompts rather than disrupts natural pain resolution processes,” she says. Diatchenko is now investigating the potential of immunotherapies that stimulate the immune system to prevent chronic pain.
Take Your Vitamins
Khan is also exploring whether a common vitamin might be part of the solution. In a pilot study of 100 patients undergoing knee replacement, his team tested the impact of taking high-dose vitamin C before and after surgery.
Encouraged by the results, Khan plans to expand the study to a 3,200-patient global trial.
“Surgery depletes vitamin C during healing,” he says. “Nearly half of patients become severely deficient, essentially developing scurvy. This increases oxidative stress and inflammation, which can injure nerves and promote chronic pain.
“Knee replacements are among the most common surgeries worldwide, yet one in five patients develop long-term pain. If supplementing vitamin C can reduce that risk, the implications could extend to other procedures, too.”
A Shift in Thinking, a Window of Opportunity
Surgery is the leading cause of chronic pain in Canada. But researchers such as Khan, Flamer and Diatchenko are optimistic that early, science-backed interventions can turn the tide.
“If lidocaine infusion can reduce chronic pain after breast cancer surgery, we could translate this to other common major surgeries, like thoracic, chest and lung procedures,” Khan says.
Likewise, if a vitamin C trial is effective in reducing chronic pain in knee replacement surgery, it could help with hip and shoulder replacements.
“Post-surgical chronic pain is an underrecognized complication that has huge economic and human costs,” says Khan. “I’m excited and hopeful because these early interventions have the potential to reduce pain and suffering for a large patient population, not just in Canada, but globally. They hold the power to reduce the substantial costs of chronic pain management, reduce opioid use and improve the quality of life for patients.” •
Professor Tania Di Renna
Women are more likely to live with chronic pain — and less likely to be believed. Inside the science, bias and push for change.
By Rebecca Cuneo Keenan
As a teenager, Mojola Omole (MD ’07) suffered severe menstrual pain. An athletic student who played forward on her high school basketball team and competed in shot put, Omole powered through the discomfort, assuming it was just a normal part of being a woman.
“My family would say, ‘Oh, Mojola always has stomach pains,’ so I just thought that was my lot in life,” she recalls. “I had anxiety and was told I ‘carried my stress in my belly.’”
It wasn’t until adulthood that Omole, now a health equity advocate and breast oncologist and general surgeon with Scarborough Health Network, was finally diagnosed with endometriosis, putting a name to the years of chronic pain she had endured.
Omole’s experience is far from unique. Women are more likely than men to live with chronic pain, suffer in silence and receive inadequate treatment.
Why Women Feel More Pain
Estrogen increases pain sensitivity, while testosterone protects against it. This makes women more susceptible to pain, says Tania Di Renna (PGME ’03), a pain doctor and anesthesiologist at Women’s College Hospital (WCH) and the medical director of the Toronto Academic Pain Medicine Institute.
Hormones can also influence how women metabolize pain medications, which can make them less effective or cause side effects. “Estrogen slows down stomach emptying, increases the body-to-fat ratio and decreases drug-binding proteins,” says Di Renna, who is also a professor in the Department of Anesthesiology and Pain Medicine at the Temerty Faculty of Medicine.
To make matters worse, many chronic pain conditions disproportionately affect women, including gynaecologic conditions such as vulvodynia, as well as endometriosis, migraine, fibromyalgia and arthritis. And only women feel the pain related to pregnancy and giving birth.
Statistics show that racialized women are more likely to experience additional effects of living with chronic pain. “Sickle cell, fibroids and endometriosis all disproportionately affect Black and racialized women,” Omole says.
A History of Being Ignored
Medicine has long dismissed women’s symptoms. Through-out history and into the 1980s, physicians often diagnosed women’s suffering as “hysteria,” as psychological rather than physical.
Studies show that women are less likely than men to be prescribed pain medication and experience the pain-relieving effects of drugs like opioids and NSAIDs differently.
This bias is mirrored in medical research on pain, which has only recently turned its lens on women. It wasn’t until 2016 that the National Institutes of Health required grant applicants to factor sex as a biological variable in the design of basic and preclinical animal research studies.
“Women’s health is underfunded, and the health of marginalized and racialized people is even more so,” says Omole.
Tatyana Mollayeva (PhD ’15 RSI), is a senior scientist at the KITE Research Institute at University Health Network. Her research focuses on the prevention and management of neurological diseases and injuries, and the role of sex, gender and intersecting vulnerabilities in shaping outcomes.
Mollayeva contends that the lack of diversity is an inherent limitation of medical research. She argues that the drive to reduce variables in studies results in homogeneous samples that can limit the usefulness of results.
“We need to pay attention to who is included in the study if we want the results to apply more broadly and improve the quality of care,” she says.
Despite the obstacles, Mollayeva is encouraged by new frameworks, such as PROGRESS-Plus, that apply an equity lens to research and account for social determinants of health such as gender, race, ethnicity and occupation.
“I think we are living in a very good era,” she says. “We have the technology that, with proper attention and ethical use, can help us understand non-linear relationships and find results that are meaningful to people.”
Mindsets Are Shifting
One area in which science is catching up is migraine, a brain disease that affects women at a rate three to four times more than men.
“As recently as the 1970s and 1980s, one of the main treatments for migraine was a medication called Fiorinal that was, in large part, a sedative,” says Christine Lay (MD ’92), a neurology professor at Temerty Medicine’s Department of Medicine and the director of the Centre for Headache, based at WCH.
The assumption was that migraine was a disorder of women who were simply stressed or overwhelmed, Lay says. That mindset has shifted. “Scientific advances have shown migraine to be a complex brain disease that can cause a moderately severe headache along with nausea, cognitive fog, light and sound sensitivity, dizziness and more.”
New targeted migraine therapies have replaced older, poorly tolerated treatments, such as antidepressants and blood pressure medication, that offered limited relief, transforming care for women living with migraine.
Pain during pregnancy and the postpartum period is also often misunderstood or minimized.
“It’s often dismissed as normal pregnancy discomfort or left untreated because of concerns related to medication safety in pregnancy,” says Rebecca Titman (PGME ’21), a physiatrist with Sinai Health’s Pain in Pregnancy Program and a professor of physical medicine and rehabilitation at Temerty Medicine’s Department of Medicine.
“Medication is only a small part of what we do to support people with pain in pregnancy,” says Titman. “Validating a patient’s pain is key, coupled with management through movement, gentle exercise, acupuncture, transcutaneous electrical nerve stimulation or mindfulness practices.”
Titman is encouraged to see the clinical community taking women’s pain seriously. As an example, she points to the growing number of pelvic health physiotherapists, which rose by 46 per cent in Ontario between 2020 and 2022.
Building a Better System
Di Renna is optimistic about recent investments in women’s health. These include a grant of almost $600,000 from the Canadian Institutes of Health Research (CIHR) awarded to Di Renna and WCH collaborators to support better screening for endometriosis. And in 2023, CIHR and Women and Gender Equality Canada supported the creation of the Pan-Canadian Women’s Health Coalition with an $8.3 million investment. The initiative established 10 virtual hubs across the country to improve the visibility and impact of women’s health research and practice.
At the same time, Di Renna and her colleagues are watching the United States, where politics are eroding scientific freedom and reproductive health research.
Omole takes inspiration from the medical learners she works with, who understand the importance of talking about misogyny, racism and marginalization.
“Systemic change is what we need,” Omole says. “But sometimes individual change is where we start.” •
Coming together to improve pain care and education in underserved communities in Canada
By Erin Howe
Centring Culture, Connection and Knowledge
Deep in northwestern Ontario, a quiet revolution has been underway in the Rainy River First Nations community. Since 2009, Elder and former Chief Jim Leonard and the Band Council have reduced drug use in the community by over 90 per cent. Their strategy included testing and enforcement, but also something less expected: listening. What they heard, again and again, was that community members were in pain.
Not just emotional pain, but the physical kind — often poorly treated, if treated at all.
What Leonard and the Band Council learned was sobering. Many community members were living with chronic pain after an injury or surgery and trying to manage with prescription drugs and other substances, which had their own risks.
Listening was the first step towards a comprehensive community-led approach to pain care, and now that innovative approach is gaining momentum with the support of health care partners more than 1,500 kilometres away.
Leonard and his team zeroed in on drug-free interventions, focusing on prevention, harm reduction, support and safety, along with housing and community care.
The stakes are high for lowering the rate of drug use. Chronic pain and substance use disorders are closely linked to higher rates of anxiety, depression and suicide.
“We estimate that within our local 350-member community, there were about 150 people using drugs, including about three-quarters of our youth between the ages of 14 and 30,” Leonard recalls, including roughly half who reported using Oxycontin. “Today, there are just less than a dozen.”
It’s a remarkable turnaround. Leonard’s Rainy River community is also part of Grand Council Treaty #3 (GCT3), the traditional Anishinaabe government that spans 28 communities from west of Thunder Bay to north of Sioux Lookout, Ontario, and along the United States border and into Manitoba.
Leonard is now sharing the Rainy River approach with other First Nations communities and municipalities.
In 2023, he helped establish the COPING Well (Chronic Pain Education for Indigenous Wellness) Project. This initiative emphasizes community-based strategies for First Nations individuals living with pain.
COPING Well is a partnership with GCT3’s Health Transformation Team and two Toronto-based partners: Ganawishkadawe, the Centre for Wise Practices in Indigenous Health at Women’s College Hospital, and Transitional Pain Service (TPS) at University Health Network’s Toronto General Hospital in its Department of Anesthesia and Pain Management.
Funded by Health Canada, the initiative takes a strengths-based approach that validates people’s experiences, supports autonomy and encourages self-advocacy. It also works to address the unique barriers that First Nations peoples often face when seeking pain care.
“Indigenous peoples have long had their health care centred around the things that are seen as ‘wrong’ with them,” says Lisa Richardson (PGME ’08), Ganawishkadawe founder and Temerty Medicine’s Vice Dean, Strategy and Governance. “Rather than focusing on deficits, we focus on people’s strengths and find ways to incorporate them into a wellness path.”
“We know from research that culture is medicine, so being connected to traditional practices and ways of knowing and healing is very protective of health. It’s about creating understanding that Indigenous peoples have so many strengths within their communities.”
In the project’s first phase, researchers invited community members to share their lived experiences through sharing circles and interviews. Together, they co-created a story map that traces the journey from pain to wellness, and new resources that explain what chronic pain is, how to live well with it and how to seek care.
The materials will soon be available in print and on the GCT3 website. The team is also finalizing companion resources for health care providers, with the aim of securing accreditation.
“There’s so much information available on cultural safety, Indigenous ways of knowing and trauma-informed care,” says Miki Peer, the COPING Well co-lead and a TPS scientific associate. “But it’s important for these principles to become embedded in curricula. Accreditation would be a great step in that direction.”
Building Anesthesia Capacity in Small Communities
As First Nations communities reshape pain care through culturally grounded approaches, members of the Temerty Medicine community are working to address another urgent need — ensuring that rural hospitals have enough anesthesia providers to keep essential services running.
A 2017 report made in collaboration with the College of Family Physicians of Canada noted that while 18 per cent of Canada’s population lives in rural areas, just eight per cent of physicians practise there. In 2019, the Canadian Anesthesiologists’ Society sounded the alarm over the growing number of unfilled job postings, many of which were in small hospitals.
These numbers are no surprise to Professor Beverley Orser (PGME ’87 & PhD IMS ’95), the chair of Temerty Medicine’s Department of Anesthesiology and Pain Medicine and an anesthesiologist at Sunnybrook Health Sciences Centre.
After she became department chair in 2017, Orser noted troubling patterns: a rising demand for locum anesthesiologists in rural Ontario, mounting surgical backlogs and the suspension of obstetrical services due to staffing shortages.
Orser worked with a team that used Canadian Institute for Health Information data to understand the landscape. The data showed that while Canada’s anesthesiology workforce was growing, it wasn’t keeping pace with population needs, and the shortfall was particularly pronounced in rural communities.
Equally concerning, says Orser, is that colleagues working in those rural areas — often family physicians with additional anesthesia training and certification — were leaving the workforce at a higher rate than their urban counterparts.
Specialist physicians certified by the Royal College of Physicians and Surgeons of Canada deliver most anesthesia care in Canada. After completing a five-year residency, these physicians are qualified to care for patients undergoing almost any type of surgery. Some complex procedures, such as cardiac, transplant or neurosurgery, require additional fellowship training.
However, in many provinces and territories, family physician anesthetists play a crucial role. They have completed an additional year of training in an accredited program and received the Certificate of Added Competency in Family Practice Anesthesia. They provide anywhere from 15 per cent of anesthesia care in Ontario to 75 per cent in Yukon.
“Access to medical care really depends on where you are in the country,” says Orser. “This is everyone’s problem. Every Canadian needs to know there is timely access to safe anesthesia care if they need it.”
To help fill the gap identified by Orser and her colleagues, Temerty Medicine offers specialty training through its Family Practice Anesthesia Program, which educates up to five learners annually to practise anesthesia care in rural and underserved communities.
As part of the program, they complete rotations in Midland, Orillia, Orangeville or Port Perry, Ontario. They are also highly encouraged and supported to participate in a five-day boot camp at the Northern Ontario School of Medicine University in Sudbury. As well, the program, in partnership with the Government of Nunavut, offers a month-long elective in Iqaluit, with the hope of welcoming back graduates as locum or staff physicians.
“The best care possible is close to home,” says Razvan Purza (PGME ’21 & MSc ’23), the director of the Family Practice Anesthesia enhanced skills program, a lecturer at the University of Toronto and a staff anesthesiologist at Michael Garron Hospital. “Where a community may not be able to support a specialist anesthesiologist due to scope or volume of work, we want to make sure care is still available.”
Purza, along with Orser and colleagues, is also working to build capacity through initiatives such as the National Pain Medicine Ground School — an annual two-day virtual boot camp that helps physicians across Canada strengthen their pain medicine skills after certification.
In rural settings, two or three physicians may support a surgical or obstetrical program or provide sedation for procedures such as gastroscopy, Purza explains. If even one provider steps away or stops practising, those services can be reduced or lost entirely.
Last fall, a Northern Policy Institute report recommended encouraging more health care professionals to pursue additional specialty skills, including anesthesia, to help address the declining access to maternity care in northern Ontario.
“What disturbs me most is that when basic access to anesthesia and pain medicine isn’t available to rural groups, it’s often Indigenous, Inuit and Métis communities who are most affected,” says Orser. “As Canadians, we shouldn’t tolerate that.”
After decades of chronic pain, Laura Swan finally found a doctor who could help. Now, as a nurse herself, she’s advocating for compassionate care.
By Laura Swan, as told to Rebecca Cuneo Keenan
I was in pain for 25 years before I found a doctor who took it seriously.
When I was young, I was trained intensively in ballet through high school, university and conservatory programs.
At 19, I injured my lower back in a fall while dancing. I remember a pop and a shooting pain, and then I was on the ground.
I didn’t take time off. I didn’t do the treatment recommended by my health-care provider. I was young — I danced through the pain.
Searching for Relief
With chronic pain, the body settles into a new normal. The pain is a constant presence in the background.
But there’s nothing normal when everyday activities hurt. I adapted. I changed how I moved. I even stopped taking deep breaths because of the pain.
When I was 30, I left dance and got serious about seeking help. I saw my GP, sports medicine physicians and an orthopedic surgeon. I consulted chiropractors, physiotherapists and massage therapists until I could no longer afford it. I didn’t have insurance and was paying out of pocket.
I was told I needed to strengthen my core to protect my back and try Pilates. And so, I did. Nothing helped.
Living Through Pain
I had two children. The pain made it hard to get a good night’s sleep. I needed time for icing and heat treatments. On long car rides we had to make frequent stops so I could get out and stretch. Chronic pain impacted my mood.
Managing appointments was challenging with an infant and a toddler. I remember a doctor telling me I needed to be in better shape — while I bounced one child on my hip and fed snacks to the other.
Every few years, I tried again. My GP prescribed cannabis for the pain, but I didn’t pursue it. Steroid shots provided some temporary relief.
Chronic pain can make you question your sanity. Maybe I’m not resilient enough. Maybe other people cope with pain better. I felt like a failure — discouraged, angry, sad.
A Breakthrough at Last
At 45, I returned to school for nursing and learned more about pain management. I knew I couldn’t go on like this for another 20 or 30 years.
I researched options and found the Schroeder Pain Assessment and Rehabilitation Research Centre (SPARC) through Toronto Rehabilitation Research Institute. I waited another year for an appointment.
They were empathetic, nurturing and understanding. But when the resident suggested allied health again, I burst into tears. “No,” I said. “I can’t do that anymore.” I asked to see the attending physician.
That doctor changed everything.
He cut through years of frustration and said: I believe you. You don’t have to live like this. We can find things to help.
An updated MRI revealed a diagnosis: arthritis of the facet joints of my spine which was irritating the nerves and causing referred pain down my hip and left leg.
I was treated with a nerve ablation procedure that uses radio frequency to cauterize the nerve and stop the pain signals. The recovery felt like deep bruising, but for the first time in over 20 years, I felt relief.
My pain, which had been an 8 out of 10 on my worst days, and a 4 on an average day, dropped to a 1 or a 2.
My spirits improved. I could sleep. I had more energy. I didn’t feel like I had to ‘grin and bear it’ anymore. I could be present for my kids.
What Medicine Needs to Hear
Now I’m a nurse, and my experience informs my practice. I’m empathetic and sensitive to expressions of pain.
I hope more health-care professionals will understand chronic pain demands more investigation, even when tests show nothing is wrong.
People living with pain are seeking compassion and validation. We under-report our symptoms. We have tried more times than you know to fix this. We are nervous to put our trust in another care plan.
People in pain are exhausted. We are desperate to be believed.
As a patient, I needed someone willing to go the distance with me until I found relief. That doctor at SPARC changed my life.
But it shouldn’t have taken 25 years to get there.
Laura Swan is a registered nurse and lactation consultant (IBCLC) who lives in Toronto with her two children.
Could a dose of hypnosis reduce post-op opioid use?
Could hypnosis help patients manage pain better after surgery and reduce reliance on opioids? A new study led by York University pain expert Joel Katz offers promising evidence for a mind-over-medicine approach.
Published in the Journal of Pain Research, the 2024 study compared patients who received brief hypnosis sessions before and after surgery with those who received standard care. The hypnosis group used significantly less opioid medication in the days following their procedures, yet reported similar pain levels, suggesting the extra opioids used by the standard care group were required to bring their pain down to a level comparable to the clinical hypnosis group.
“Prior studies indicated that clinical hypnosis can effectively alleviate post-surgical pain, but there is limited information on its impact on opioid use,” says Katz, a Distinguished Research Professor of Psychology with York University.
“We hypothesized that reducing opioid intake — without increasing pain intensity — could give patients a head start, ultimately aiding them in reducing their reliance on opioids sooner and facilitating a quicker, less painful recovery.”
The study involved 92 adults undergoing cancer-related surgery at Toronto General Hospital (TGH). Half received standard care, while others participated in two 30-minute hypnosis sessions focused on relaxation, visualization and physical comfort, but not on reducing medication.
“Most patients and doctors prefer to avoid opioids when possible, provided there are other effective options,” says Katz, who is also a professor in Temerty Medicine’s Department of Anesthesiology and Pain Medicine. “Clinical hypnosis appears to be one such low-cost, effective approach.”
Katz was surprised that the results were not a pronounced as anticipated, something he attributes to a “low dose.”
“Patients had just two hypnosis sessions, with just one given after surgery when they were experiencing pain. A more intensive treatment protocol, such as daily postoperative hypnosis, might yield more significant results,” he says.
Beyond lower opioid use, hypnosis patients reported significantly less “pain catastrophizing”— a negative, anxious mindset about pain — one week after surgery. This psychological benefit may be especially important for patients at higher risk of chronic pain or opioid dependence. There were no significant changes in sleep, mood, or anxiety, likely because participants reported low levels of pre-surgery distress.
With further research underway, Katz and coauthors — including study co-lead Aliza Weinrib, a clinical health psychologist at TGH’s Transitional Pain Service, and collaborators from the Toronto Academic Pain Management Institute (TAPMI) at Women’s College Hospital and the University of Calgary — are now exploring which patients might benefit most and how to optimize clinical hypnosis delivery.
“One upcoming study will test a higher ‘dose’ of clinical hypnosis after surgery,” says Katz. “We’ve also begun research on hypnosis for gastrointestinal symptoms — such as nausea, vomiting, and bloating — experienced by some patients with Ehlers-Danlos Syndrome to evaluate whether we can alleviate these symptoms and enhance quality of life.”
Cruel clockwork of cluster headaches
“These aren’t migraines with a twist,” says William Kingston (PGME ’16), a neurologist and headache specialist at Sunnybrook Health Sciences Centre. “Cluster headaches have a distinct rhythm and ferocity. The pain is often described as the worst a human can experience.”
Affecting just 0.1 per cent of the population, cluster headaches are rare but debilitating. Nicknamed “suicide headaches,” they strike with clockwork precision — as many as eight times a day — and are marked by stabbing pain and autonomic symptoms such as red eyes, nasal congestion and drooping eyelids on one side of the head. Most attacks occur at night and last less than three hours, making them difficult to treat and even harder to diagnose.
“They have extraordinary predictability — often occurring at the same time of day or same time of year,” says Kingston, a neurology professor in Temerty Medicine’s Department of Medicine.
Another hallmark is restlessness. “My patients describe pacing, rocking, even banging their heads against the wall or jumping into a snowbank during an attack,” he says. “People experiencing migraine want to lie down. But for people with cluster headaches, the pain is so intense, they can’t sit still.”
Because symptoms can resemble more common conditions like migraine, allergies or dental pain, diagnosis is elusive. Only 20 per cent of patients receive an accurate diagnosis within five years of symptom onset, and some go decades without answers. The episodic nature adds complexity. “Cluster headaches may appear for six weeks of the year and then vanish entirely,” Kingston says.
The pain can be life-altering. More than half of patients report suicidal thoughts. Others develop anxiety or cephalalgiaphobia — the fear of future headaches.
Standard migraine medications are ineffective or impractical, and the short, frequent attacks make dosing a challenge. Fast-acting treatments like high-flow oxygen and injectable or nasal spray triptans, such as zolmitriptan, remain first-line options.
But new tools are emerging. Preventative treatments now include oral steroids and galcanezumab, a CGRP monoclonal antibody, which was approved for cluster headache prevention in Canada in 2021. “Occipital nerve blocks have strong evidence, and can be done in office,” Kingston says. “Whatever we can do to shorten the attack duration or reduce the number of headaches helps reduce the burden of this disease.”
Non-traditional therapies are also emerging. Vagus nerve stimulation offers a drug-free alternative, and early-stage research into psilocybin microdosing is drawing attention.
“Psilocybin needs to be fully evaluated before we can recommend it, but early results look promising,” Kingston says. “The future of cluster headache care may look very different from what we imagined even five years ago.”
For Kingston, progress means more than new therapies. “Headache disorders are often invisible and heavily stigmatized,” he says. “But in headache medicine, you can really change people’s lives.”
For many, a vaccination isn’t just a little pinch — it can trigger fear, nausea, dizziness and fainting. For children, who receive most routine vaccines early in life, a bad experience can lead to long-term fear and even avoidance of medical care altogether.
“Pain and fear undermine vaccination,” says Anna Taddio, professor at the University of Toronto’s Leslie Dan Faculty of Pharmacy, and senior scientist at Toronto’s Hospital for Sick Children (SickKids). “These early experiences can have a ripple effect that lasts a lifetime.”
In Canada, one in four adults reports a fear of needles, and 10 per cent say that it affects their decision to be vaccinated. Taddio studies how to reduce procedural pain during vaccination which improves vaccination experiences, and in turn, builds trust in healthcare.
Enter CARD — an evidence-based system designed to address needle fear and discomfort head-on. CARD was developed by Help Eliminate Pain in Kids & Adults, a multidisciplinary group from across Canada led by Taddio.
Originally piloted for use in school vaccination programs, CARD — short for Comfort, Ask, Relax, Distract — offers a menu of supports that gives people a say in how they experience their vaccinations or other needle procedures. They “play their cards” by choosing strategies like having a support person present, asking questions to allay concerns, deep breathing to calm themselves and bringing along a distraction to divert their attention to something positive.
Early results proved promising. In a controlled study involving 10 schools in Niagara, Ontario, students using CARD reported less fear and dizziness. The findings appeared in Paediatrics & Child Health in 2019.
“We saw a real shift in how kids felt,” says Taddio. “They were more informed, more engaged and more at ease.”
Drawing on subsequent studies involving over 20,000 vaccine recipients across the lifespan and getting vaccinated in diverse settings, CARD is proving to be low-cost, easy to implement and highly effective.
The CARD System has now grown into a full digital hub hosted on the SickKids AboutKidsHealth site. The site is packed with videos, posters, handouts and interactive tools, like a digital game that walks players through a maze to collect comforting items like teddy bears and blankets.
The hub also offers age-appropriate scripts to help caregivers and clinicians talk to kids in honest and coping-promoting ways — for example, swapping “This won’t hurt” for “Some people say this feels like a pinch or pressure, and others say it doesn’t feel like much. Let me know what it feels like for you.”
The CARD resources are freely available for everyone to use, including organizations and providers delivering vaccinations and individuals getting vaccinated.
“We now have a way to take fear out of the equation,” says Taddio. “It’s time we started treating pain as a side effect of vaccination and preventing pain as an essential part of good vaccination practice.”
Protecting the brain to tune out pain
Why does pain affect people so differently? For neuroscientist Karen Davis (PhD ’88), the answer lies in how the brain processes nociceptive signals — and could lead to more effective, personalized treatment.
“Pain isn’t just a sensation,” says Davis, a senior scientist at University Health Network’s Krembil Brain Institute and Canada Research Chair in Acute and Chronic Pain Research. “It’s about how the brain perceives, processes and regulates nociceptive signals, and that varies from person to person.”
Davis has spent decades studying the brain networks underlying pain and its modulation. Her pioneering research includes some of the first functional MRI images to show how individuals experience the interplay of pain, cognition and attention during focused tasks. Her findings revealed that while some people can ignore pain and stay focused, for others, it overwhelms their ability to function.
Davis is particularly interested in the brain’s default mode network — a set of regions typically active during rest and self-reflection. In people with chronic pain, these areas appear more tightly linked, especially those involved in self-referential thought. “This may explain why people often ruminate on their pain,” she says. “They simply can’t tune it out.”
Knowing that pain is processed differently from one person to the next may also explain why pain treatments don’t work equally well for everyone.
Now, Davis, a professor at Temerty Medicine’s Department of Surgery and Institute of Medical Science, is working to identify brain- and behaviour-based biomarkers that could help predict individual pain responses, and which treatments could be most likely to help.
In one line of research, a simple 10-second test gauges pain sensitivity and whether a person’s brain chemistry suggests they might respond to a specific medication, such as an infusion of ketamine, which is an NDMA antagonist. Another test assesses how well the brain suppresses pain, offering clues about whether interventions like cognitive behavioural therapy, mindfulness or transcranial magnetic stimulation might be effective.
“Many patients cycle through treatments without success,” says Davis. “It’s exhausting for them, and expensive for the healthcare system. Personalized care could change that.”
Can we talk about pain?
Once seen as a symptom, chronic pain is now recognized as a disease in its own right. Yet, despite its prevalence, pain can be tough to communicate about. Meet a podcaster, a YouTuber and an educator from Temerty Medicine community who are breaking the silence and changing how we talk about pain.
Professor Hance Clarke
By Heather McCall
Sandra* suffered a traumatic accident that required major surgery. Discharged with a prescription for opioids and reassurance that her pain would gradually subside, she instead suffered lingering nerve and muscle damage that left her with chronic, debilitating pain.
With little follow-up care, Sandra managed alone. She gradually increased her medication use, unaware that she was becoming dependent. What began as temporary pain relief became a struggle with opioid use disorder.
A decade ago, this experience was all too common. While most surgical patients recovered without complications, 15 to 20 per cent developed chronic post-surgical pain.
Today, however, pain management experts such as Hance Clarke (MD ’03, PhD ’13 & PGME ’08) are helping people break free of the post-surgery pain cycle while reducing the risk of opioid use disorder.
Clarke’s passion for pain care was sparked by a deeply personal experience. During his final year of high school, his father was nearly killed in a devastating accident at work. As a family, they endured the aftermath of multiple life-altering procedures, exposing Clarke to the complexities of post-surgery recovery.
Now a leading clinician-scientist specializing in anesthesiology and pain medicine at the Temerty Faculty of Medicine and University Health Network (UHN), Clarke has dedicated his career to finding solutions for patients who might otherwise slip through the cracks.
One of his early accomplishments came in 2014, amid the growing opioid crisis.
Clarke’s research showed that proactive, interprofessional care could significantly reduce opioid dependence and improve recovery. This led Clarke to spearhead the Transitional Pain Service (TPS) at UHN’s Toronto General Hospital.
TPS’ interprofessional program identifies high-risk patients before and after surgery. It offers early interventions to keep pain from escalating, combining medications with psychological and physical therapies.
“We can now interrupt behaviours and change the trajectory of a patient’s pain,” Clarke says. “Instead of waiting until they are dependent on opioids, we give them the right tools from the start.”
The TPS model has since expanded across Canada and is now being studied and adopted internationally.
Over the past decade, Clarke has turned his attention to policy. With the University of Toronto’s Centre for the Study of Pain, he has helped shape national opioid prescribing guidelines and is investigating cannabis as a therapeutic, non-opioid treatment.
His team’s recent findings suggest that tetrahydrocannabinol (THC) may act as a disease-modifying agent for osteoarthritis — an insight that could revolutionize non-opioid options for chronic pain care.
With cannabis research still gaining traction in medical circles, Clarke is advocating for drug identification numbers for cannabinoid-based therapies — an important step toward their acceptance in mainstream medicine.
“Opioids were the king of pain medication for decades, and they overshadowed other pain management strategies,” he says. “We need to rethink how we approach chronic pain and integrate new therapies backed by science rather than habit.”
As the president of the Canadian Pain Society (CPS), Clarke is raising the profile of chronic pain as a distinct medical condition. Despite affecting 20 per cent of the population, chronic pain research received just 3.2 per cent of global health care funding at its peak in 2019.
Under Clarke’s leadership, CPS is pushing to make pain management a public health priority, mobilizing researchers, policymakers and patient advocates.
Looking ahead, Clarke sees the integration of mental health and pain management strategies as the next big frontier. His recent appointment as a research chair at the Centre for Addiction and Mental Health (CAMH) underscores his commitment to developing integrated care pathways.
By fostering collaborations between institutions such as UHN and CAMH, Clarke hopes to redefine chronic pain care at a systemic level.
“Pain isn’t just physical — it’s deeply intertwined with mental health,” Clarke says. “If we continue to treat them separately, we’re missing half the picture.”
“At U of T, our leaders are well positioned to drive the integration of policy and funding. Together, we have the opportunity to improve care — and quality of life — for the eight million Canadians who suffer daily with chronic pain.” •
*Composite patient based on clinical experience
Professor Neil Goldenberg
By Emma Jones
Early support gives new clinician-scientists the tools to cultivate careers
Launching a career as a clinician-scientist — a physician who both cares for patients and pursues research — is notoriously challenging. These new physicians are responsible for the health and well-being of multiple patients. At the same time, they must establish a research lab and hire staff, which requires significant funding and precious time.
“When you’re done your training and start to work independently, it’s stressful. Now it’s your name on the door, and what goes on in that room is your responsibility,” explains Neil Goldenberg (PhD ’09 IMS, MD ’11 & PGME ’18), the inaugural John Alchin and Hal Marryatt Early Career Professor in Anesthesiology and Pain Medicine at the Temerty Faculty of Medicine. “And to also launch a research lab, you need protected time to be able to do your work, and you need a considerable amount of startup money to be able to get going.”
It’s a tall order, but one worth tackling, says Goldenberg. While clinician-scientists make up less than two per cent of the world’s physicians, their dual focus has an outsized impact in driving new advances in health care.
It’s an appreciation shared by Temerty Medicine alumnus and former faculty member Hal Marryatt (PGME ’71) and his husband, John Alchin (MBA ’79). In 2021, the couple made a gift to establish a namesake professorship in anesthesiology and pain medicine at Temerty Medicine. Specifically designed to support clinician-scientists in the first years of their career, the position provides the time and resources critical to launching a successful career in academic medicine.
“We wanted to give a boost to those building a body of work that would allow them to access funding pools for more established researchers and build future careers,” explains Marryatt, who worked as a resident and then staff anesthesiologist in the Respiratory Failure Unit at University Health Network’s Toronto General Hospital.
As Alchin explains, supporting pilot projects and professionals early in their careers is a tried-and-true approach.
“We both like the idea of supporting a person or a project at the beginning of the career and giving them a boost up, so they can spend more time focusing on development and less time trying to raise money.”
For Goldenberg, the first to hold the named professorship, the position has allowed him more time to focus on his research and clinical duties rather than filling out grant applications. It has also helped open doors to further support by demonstrating institutional trust in his work.
Goldenberg’s lab studies pulmonary hypertension, a severe lung disease affecting the lung’s blood vessels. The condition has a high mortality rate, and patients are especially vulnerable to complications from anesthesia. Goldenberg and his team are investigating the immune system’s role in the disease’s development. Their goal is to seek new ways to treat the condition before surgery is needed.
“This support made a real difference to the budget of my lab and to what research goals we could pursue,” Goldenberg says. “Equally important was the credibility that it gave me. When you transition beyond early-career support, you’re suddenly competing against other researchers who have 20 to 30 years of experience in the field. It’s incredibly daunting but here, I had a professorship that gave me validity.”
Goldenberg’s time in the early-career professor role was cut short in the best way possible. Before the end of his term, he was awarded the Wasser Chair in Anesthesia and Pain Medicine at The Hospital for Sick Children — a testament to the power of early-career investment. This new role allows him to continue his pulmonary hypertension research.
For Marryatt and Alchin, Goldenberg’s success affirms their decision to support clinician-scientists early on. They are now supporting a second early-career professor and looking forward to seeing where this new researcher, soon to be named, will take their career.
“It was really inspiring just to see the success Neil had and to see what he’s going on to,” says Alchin. “That plants the seed, ‘Wow, it would be great to do that again and find another candidate who could take advantage of the opportunity and go on to something bigger and better from there.’” •
Source: Toronto Star
A step back in pain relief history
Long before the advent of modern pain clinics, people from around the globe lined up for a different kind of clinician: Dr. Toe-Twister.
Otherwise known as Mahlon Locke, he studied at Queen’s University’s School of Medicine in Kingston and then completed a fellowship in Scotland. In 1908, he returned to Ontario to open a family practice in Williamsburg, a village near Brockville.
Convinced that arthritic pain stemmed from fallen arches, Locke gained fame for his unorthodox treatment approach. He manipulated different parts of his patients’ feet with a toe-twisting technique that he claimed realigned the body and relieved everything from headaches to back pain.
Throughout the 1920s and ’30s, “Dr. Toe-Twister” treated thousands of desperate patients at his village clinic. Some came on crutches and reportedly left dancing. Combining chiropractic techniques with a flair for theatrics, Locke inspired the public but drew skepticism from the medical establishment.
At a time when science offered few answers for chronic pain, Locke offered hope for its relief.
Modern clinicians share Locke’s goal of easing pain, but today, evidence-based research, advanced diagnostics and interprofessional care have transformed our understanding of pain management and improved outcomes.
Still, Dr. Toe-Twister’s legacy endures. It reminds us that healing is more than technique. Whether in a village clinic or modern hospital, trust and empathy remain the cornerstones of care. •