The Avatar
We Asked …
What will medicine look like in 20, 50 or even 100 years? Will microscopic cameras rove through our bodies, uncovering cancer cells and killing them on the spot? Or will disease be a distant memory, its genetic roots long since programmed out of the human race?
Will it be impossible to tell where flesh ends and bionics begin? Will we find a cure for aging — or run out of land and water and become a spacefaring species?
In the following pages, we asked professors and alumni from every part of the Faculty of Medicine to predict our medical future, both near and very far. We hope you are inspired by their ideas.
The Avatar
In 100 years, we’ll all have avatars made up of our own cells. Medical procedures will be performed on them first to see the real consequences in real time. This will open a whole new field of medical bioethics — where does the person end and the avatar begin?
—
Professor Alison Buchan, Vice-Dean Research and International Relations.
The Unknown Maladies of a 150‑Year-Old Brain
In 20 years, I hope that in the area of mental health and addiction, diagnosis will be much more specific, with the help of neuroimaging, genetics and biomarkers. I expect we’ll also have a much better understanding of the role of epigenetics and how environmental experience influences gene expression. All of this should allow us to find the “sweet spot” between therapeutic effects and unwanted side effects in medications.
I think we’ll be able to make excellent use of neuromodulation interventions targeting specific areas of the brain causing illness. We’ll know how to tailor psychological and psychosocial therapy and provide interventions and help through smartphones and other mobile devices. We already have texting-based psychotherapy that seems to work. And as this trend continues, we’ll gather a massive body of evidence about the kinds of therapeutic approaches that work and why one provider is achieving more success than another.
We also hope to understand much more about neuroplasticity and how damaged brains can heal. And in an ideal world we’ll be able to identify and repair the genes that cause schizophrenia before it starts.
But with the kinds of medical advances on the horizon, you never know how psychiatric needs will change. Nobody anticipated we would face so much dementia, and that’s because we’re living longer.
—
Molyn Leszcz is Interim Chair of the Department of Psychiatry and Psychiatrist-in-Chief at Mount Sinai Hospital.
↓
Star Trek Got It Right
The price we pay for evolution and natural selection is cancer. Genetic mutations may cause cancer, but they also have allowed humanity to progress — without it, we’d still be living in the swamp. I don’t see cancer disappearing for this reason alone, whether in 20 or 100 years.
However, our capacity to detect cancer has skyrocketed in the past few decades — and the rise of Big Data will only speed up this progress.
It’s amazing to think we didn’t have CT, MRI and PET scans just four decades ago. And yet, in 20 years, people may laugh at us for using radiation to look into the human body. When that point comes, when imaging is totally non-invasive, then everybody will be imaged.
Star Trek got it right: the first thing you do is scan the patient to find out what’s wrong. Every door to a hospital will have an MRI scanner, and you don’t walk into a medical appointment without a full body scan. Diagnosis and therapy will be in the same space: use a tracer to find the tumor, but tag that tracer with therapy to treat it simultaneously.
By 50 years, you’ll be scanned and if a buzzer goes off, that means they found the tumor. Computers will do most of the scan analysis — they’re better at recognizing patterns. “Texture analysis” will be used routinely. Even now, satellites can see one person in a military operation, and can look under water and rocks. That’s the same technology we’ll be using.
In 100 years, radiology won’t exist as we now know it. We can’t fight against evolution, but we can at least try to repair the damage. We’ll be sending in nanotechnology to bandage up your DNA. As a result, we’re probably looking at lifespans of 120 years.
—
Alan Moody (PGME ’91) is Chair of the Department of Medical Imaging and Senior Scientist, Physical Sciences, Schulich Heart Research Program, Sunnybrook Research Institute.
Stem Cellborg?
In 20 years, stem cells will at least partly restore vision; and the combination of biomaterials and cells will enable us to use personalized medicine to better predict which drugs will be useful for any person.
In 50 to 100 years we’ll be programming the disease right out of people by manipulating their cells. Humans will be more integrated with electronics, leading to bionic people.
I’m most excited about combining stem cells and delivery vehicles. We’ve invented materials that allow you to inject cells where you want them to be, like the back of the eye or in the brain. These materials promote the survival of the cells in these new locations. The eye is so promising because the retina is a defined space and we know which cells to replace. The brain is much more complicated in terms of which circuits have to be reconnected in order to regain function.
→
Molly Shoichet is Senior Advisor on Science and Engineering to U of T President Meric Gertler. She holds the rank of University Professor, with appointments in Engineering, Medicine and Arts and Sciences.
—
Starvation, Plagues and War
In the next century we may have the technological potential to keep the average person alive past 100, but it won’t happen.
What keeps us alive is air, water and food.
Farmland destruction and population growth will lead to food shortages worldwide. Population growth is fastest in parts of the world without stable governments or health care systems. Access to water, food and land will cause wars between nations.
The obesity problem will disappear, but there will be plagues of uncontrollable bacteria for which we’ll have no antidotes because of the widespread overuse of antibiotics.
For Canadians, there is a way forward. As the world warms, huge swaths of farmland may open up in northern Canada. We will need to create and use genetically modified sources of foods.
G. Harvey Anderson is Executive Director of the Centre for Child Nutrition, Health and Development, and a Professor of Nutritional Science and Physiology.
No Cure for the Common Death
In 20 to 50 years, I don’t think we’ll see significantly extended lifespans, despite advances in medical research. This is for social reasons: effective immortality would be incredibly selfish to future generations and we’d simply stagnate without the turnover. But there will be improvements in health such as Artificial Intelligence Immunity, which will be capable of bolstering the immune system through surveillance and eradication of damaged cells and infections. Such designer immunity may make antibiotics irrelevant by supercharging our own immune systems.
The biggest challenges in the developed world will be obesity, lack of exercise and mental illnesses. These won’t be overcome by medical innovation but by social restructuring.
We tend to overestimate progress in medicine. The hard part is always the implementation. For example, genomics has enormous positive potential — but this will be for nothing unless the public trusts that their genomic data won’t be used against them. I see this as a major problem in the next 20 years as we realize privacy and trust can never be guaranteed.
In 100 years, hospitals as we know them won’t exist. We’ll still have medical needs but these will be provided by smaller, specialist “hotels.” Chronic care will be provided autonomously, including through life-sustaining mobile machines. Quality of life will be better appreciated and people will have far greater say in their fate. Physician-assisted death will evolve into patient-empowered end-of-life care.
I’m most excited about the development of CAR T cell therapy (a type of immunotherapy), which is enormously promising for cancer treatment but will probably be adapted to broader uses.
—
Jim Woodgett is a Professor in the Department of Medical Biophysics and Director of Research at the Lunenfeld-Tanenbaum Research Institute, Mount Sinai Hospital.
Sky’s the Limit
I wouldn’t be surprised if bionics becomes a reality. For that matter, are humans going to be a species that remains on earth forever, or will humans become a spacefaring species? Our imaginations shouldn’t have limits.
↑
Former astronaut Dave Williams is an Assistant Professor of Surgery at U of T and President and CEO of Southlake Regional Heath Centre.
The Future Is Here — But It’s Stuck in Trials
Today, we’re treating the disease. In 50 years, we’ll be treating the person’s manifestation of disease, based on her genetic and other health information. But when will this precision medicine come to the patients of Ontario? Unless our health care system creates the capacity to use this information, we’ll fall behind. We are already falling behind.
Medical imaging, advances in biological science and developing the technology to deliver it are moving at a fair clip. It’s blending it all that will help us to realize a time when disease can be treated as just an irritation, to be brushed away like a pesky fly; when genetic aberrations are identified and fixed at birth.
Our ambition has to be systemic. University teaching has to be in tune with the medical landscape. Government has to recognize our need to speed up the glacial pace of progress.
And the public has to let us in. We will ask them to participate in this health care revolution, to let us collect the biological, imaging and other needed information to realize our ambition. We need hundreds of thousands of data points for every question we ask. We need multiple millions for a disease-free future.
Getting there is not the job of one hospital or one health care system. It’s the job of each and every one of us. It’s the job of the world.
—
Michael Julius is Professor of Immunology and Vice-President of Research at Sunnybrook Health Sciences Centre.
Rising Above Our Bodies
In 50 to 100 years, I can imagine touch screens operated with the eye or the mind! The physical body will be less and less important — it will become an accessory. There might be “body clubs” where hobbyists go to use their bodies for nostalgic or other specific reasons, just as now there are still photographers who develop film in a darkroom for specific effects.
Health providers will be more like mentors, empowering the individual to create a meaningful and purposeful life. For example, maybe in rehabilitation sciences, we’ll be giving you what you need to climb mountains bionically.
Right now, our bodies keep us down. We spend so much time and energy trying to keep our bodies healthy, but in the future machines will do that. A machine will print a new knee, a better heart. Taking care of bodily problems will be mundane.
Think of Stephen Hawking. His body traps him — it’s worse than useless. But if you think about what his mind is doing, he’s probably the most able human being alive.
→
Helene Polatajko (MEd ’78, PhD ’82) is a Professor in the Department of Occupational Science and Occupational Therapy and Interim Director of the Rehabilitation Sciences Institute.
Follow the Money
I wouldn’t dream about genomics and drugs because progress is so slow, and the cost of drug development doubled to an average of $2 billion per medication in just the past two decades.
The structure of DNA was discovered in 1953. Today, we don’t have genetically engineered monkeys running around doing work for us. Gene therapy is still a dream for the most part. We’re still attacking autoimmunity with the same framework we did 50 years ago. The truth is we don’t have the financing or the science to properly support drug development. It may take a full 100 years, or more, for the optimism about the usefulness of genetic sequence information to pay off in a practical way that is evidence based.
But the medical device world operates on a completely different life cycle. The cost of sensor technology, in particular, is coming down. We’ll use it to record massive amounts of lifestyle information that will be the most immediate and perhaps most important future of Big Data in medicine.
Within 20 years, wearable technology is going to break out of the niche fitness market and explode for managing chronic diseases like Parkinson’s and MS. It will be as pervasive as the Internet. This could start very soon if smartwatches (e.g., Apple Watch) take off.
In 50 years, we’ll be synthesizing data from our whole lives — heart rate, exercise, blood sugar and millions of other data points. We’ll have our own personal life data series of all our responses to food, entertainment, the personal relationships that cause anxiety. This will lead to preventative medicine on a level much more sophisticated and finely textured than telling people to eat right and exercise. What triggers a migraine for you? What’s your risk of heart attack based on how much you’ve been sitting lately? The data explosion will completely recast personalized medicine.
This will lead to a sea change in our society. Insurance companies will rise in power, and may displace technology companies to become the largest firms in the world. They will support a wearable outpatient system that will provide them with real-time updates on your lifestyle habits, which they will use to update their risk models of you and adjust your premiums. Physicians are neither equipped nor paid to analyze all this data, so an entirely new industry of privately funded analysts will spring up.
The end result: Right now the medical system is organized around hospitals and focused on treatment. In the next century, it will shift to the private sector and prevention.
↑
Jayson Parker (BSc ’91, MSc ’93, PhD ’99) trained as a neuroscientist and worked as a stock analyst in the health sciences. Currently, he is a biotechnology lecturer in the Department of Biology (UTM), Faculty of Law and at the Institute of Biomaterials and Biomedical Engineering. He also serves as an adviser to a hedge fund.
—
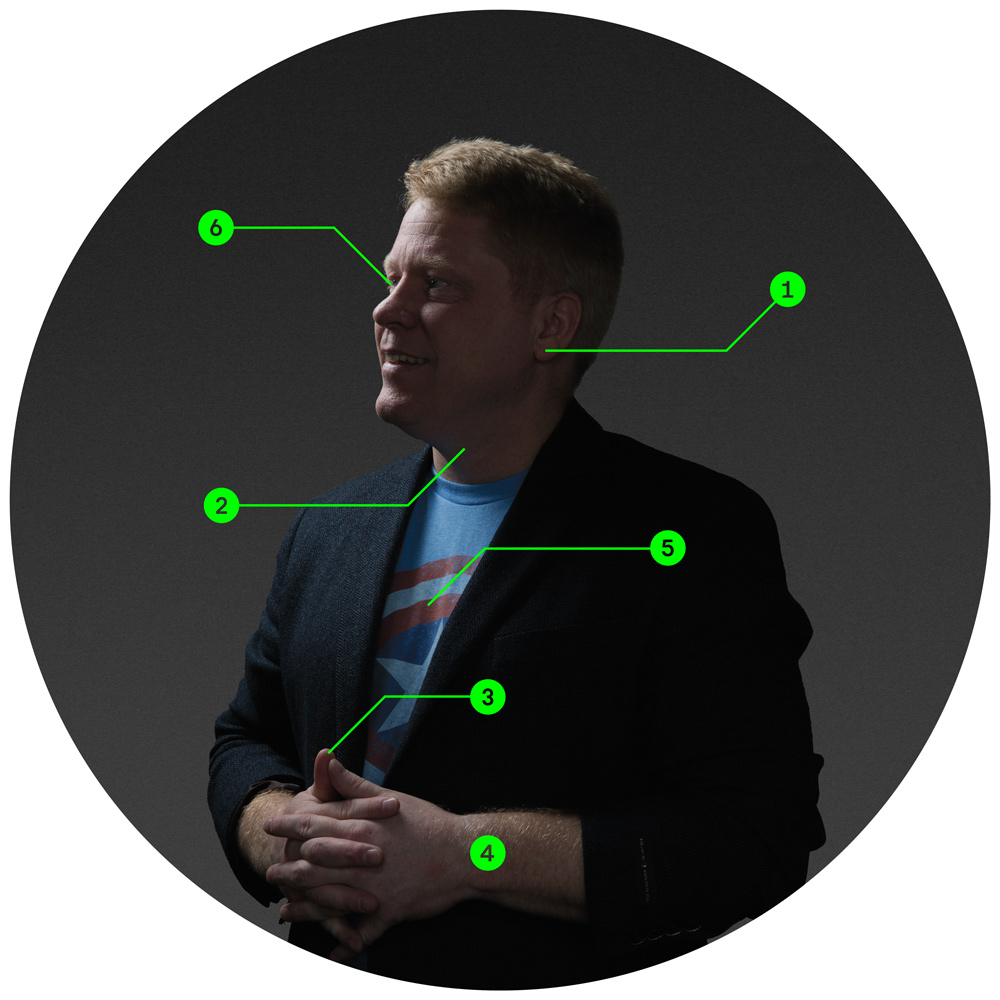
Wearables of the Future
1. Earlobe — blood glucose monitor
2. Necklace — responds to swallowing action in an effort to track food consumption
3. Thumb — tattoo that scans for toxins and viruses
4. Wrist — Fitbit and the AppleWatch
5. Shirt (Hexoskin) — measures breathing volume and heart rate
6. Eye — contact lens displays health data
The Importance of a Sheep
I don’t think the end of disease will happen anytime soon. I don’t think we know enough about the cellular equipment and how to fix it. The human system isn’t engineered. We were put together ad hoc over a billion years, and we’re still learning about the layers of complexity that need to be uncovered.
Because people developed so haphazardly, maybe it’s no surprise that the greatest medical discoveries have come by accident, often when scientists were looking for something else. I work in genomics and computational biology, but the big moment for me in science wasn’t the decoding of the human genome or the explosion of Big Data. It’s when we cloned Dolly the Sheep. That achievement went against expectations because it showed that genetic programs are much more malleable than anybody thought.
—
Tim Hughes is a Professor with the Donnelly Centre for Cellular and Biomolecular Research.